Member of the American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS)
Exophthalmos and Enophthalmos
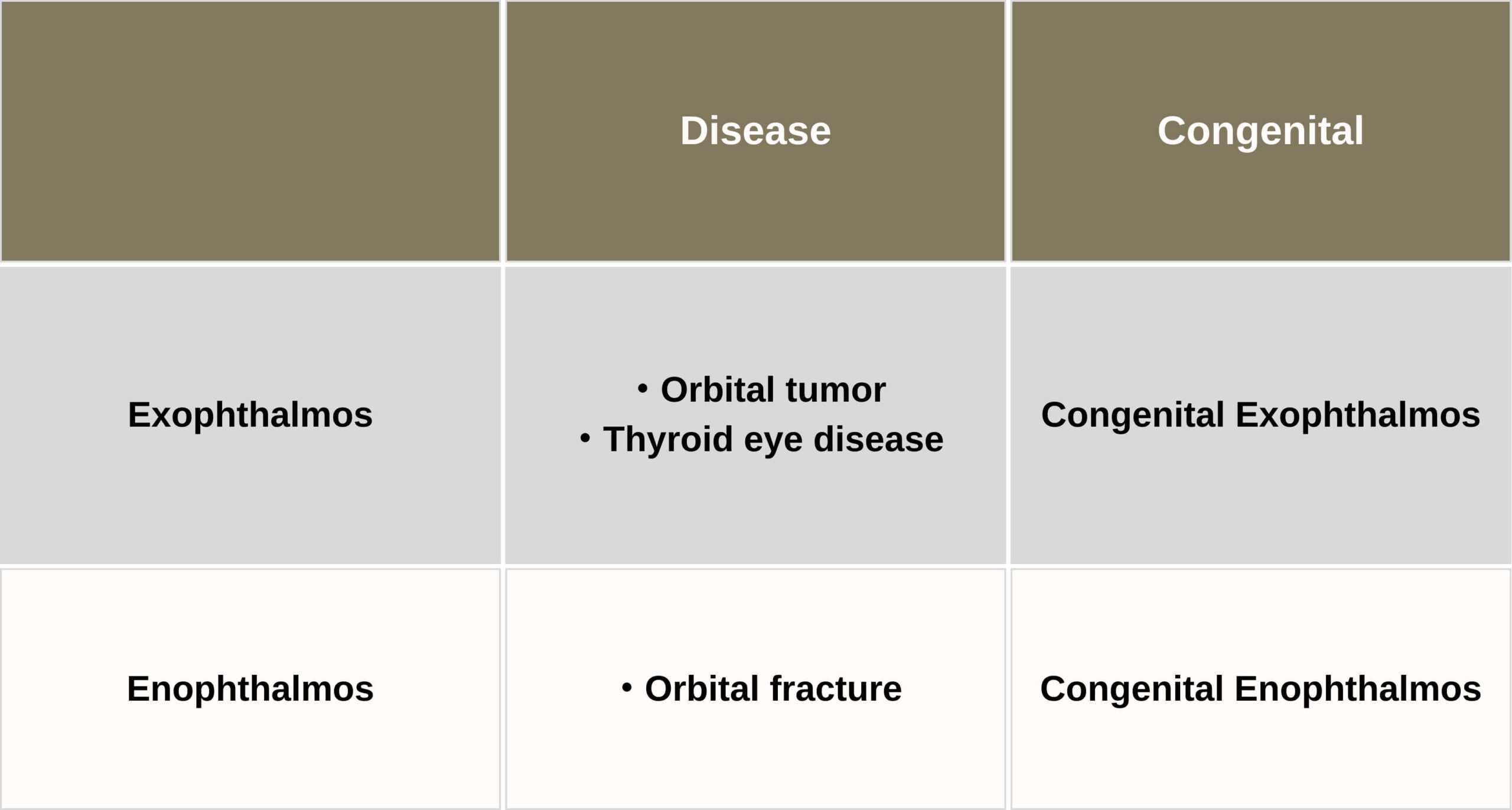
There are two types of cause for each.
One is condition from illness and the other is by nature. Aesthetic Orbital Surgery treats these patients aesthetically.
4 types of conditions
So there 4 types of conditions. We are treating those patients respectively.
Exophthalmos
For exophthalmos, 3 types of condition.
Orbital tumor
Thyroid eye disease
Congenital exophthalmos
Orbital fat decompression for thyroid eye disease and congenital exophthalmos
Let’s move on to orbital fat decompression.
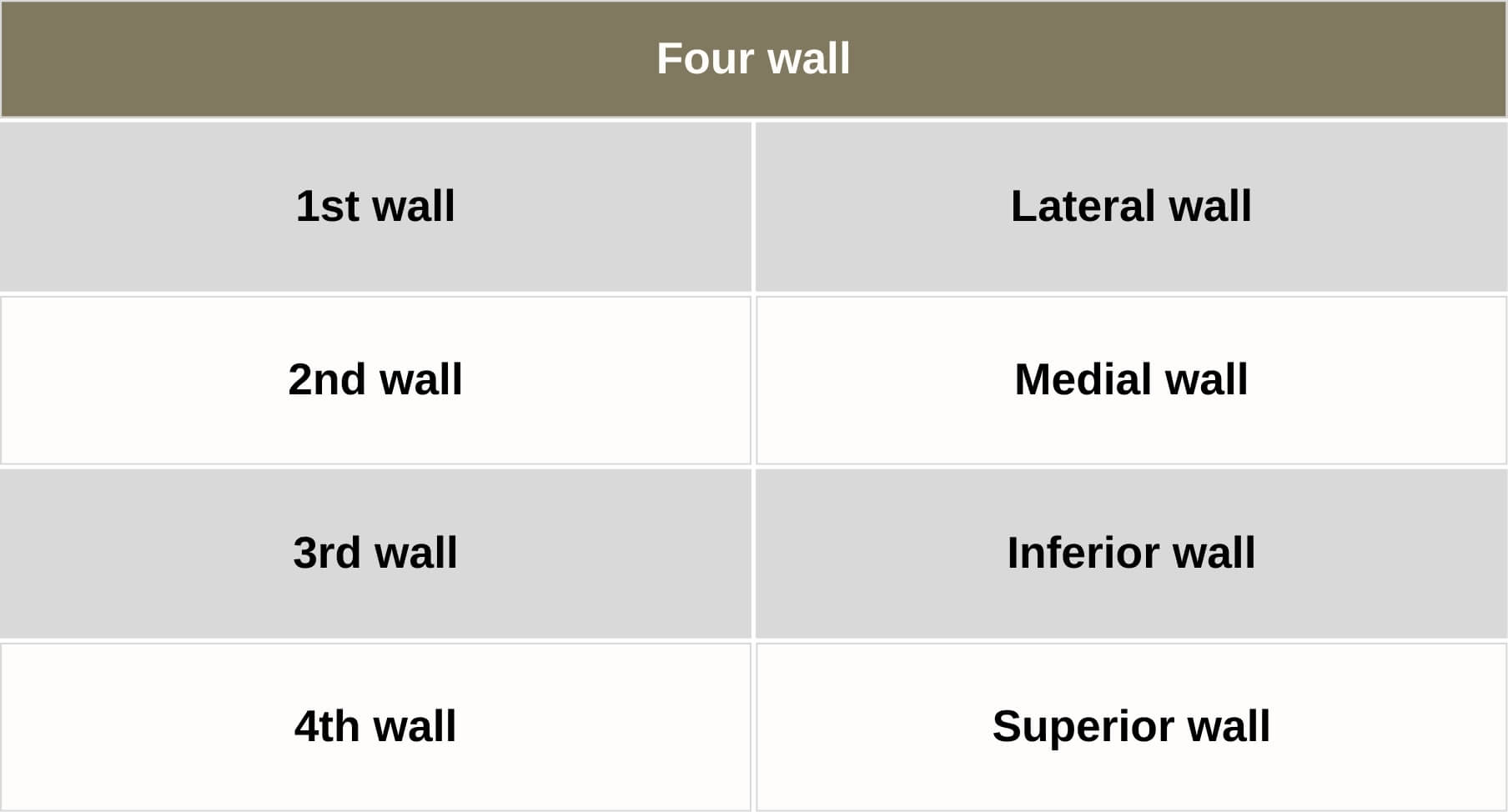
Orbital bone decompression
From orbital anatomy the four walls surrounding orbital tissue (lateral /medial /floor /roof) can be decompressed.
The decompression of each 4 walls have each benefit and risk.
The risks of BONE decompression
We must think about the risk of Bone decompression. It is the damage to surrounding tissue outside and inside of bone, such as, brain, nerves, vessels and nasal cavity.
The most serious problem is brain injury. The surgeons feel fear for fatal event.
And this method have relatively high probability of new onset diplopia.
But…
Bone doesn’t play any role in TED
Increasing volume of fat (and/or muscle) have important role for proptosis
Ideally, the target should be something different.
Fat decompression is 5th wall decompression. He reported new onset diplopia occurs 2.5% of cases.
Advantage of FAT decompression compared to BONE decompression
Natural
No skin Scar
Short recovery
Predictable and adjustable
So, why I changed my first choice from bone to fat?
Fat decompression have 4 advantage comparing with bone decompression. It can create Natural form, without Skin Scar, Recovery time is short and the result is predictable and adjustable.
However…
However, Posterior orbit is so dense with muscle, nerves and vessels.
Removing only fat seems like an impossible task.
So, I will tell you how I remove orbital fat without damaging those important tissue.
To avoid the complication we use 2 tools
Microscope(Leica M320)
We always use microscope for orbital fat decompression. Leica M320 is made for dentists. It is so good for oculoplastic surgery and also cheap.
It costs about 30,000 US. One fifth of normal microscope for ophthalmologists.
The microscope is necessary for orbital fat decompression especially for intraconal fat resection.
Spatula
And spatula is good tool for invading deep orbit without damaging important organ.
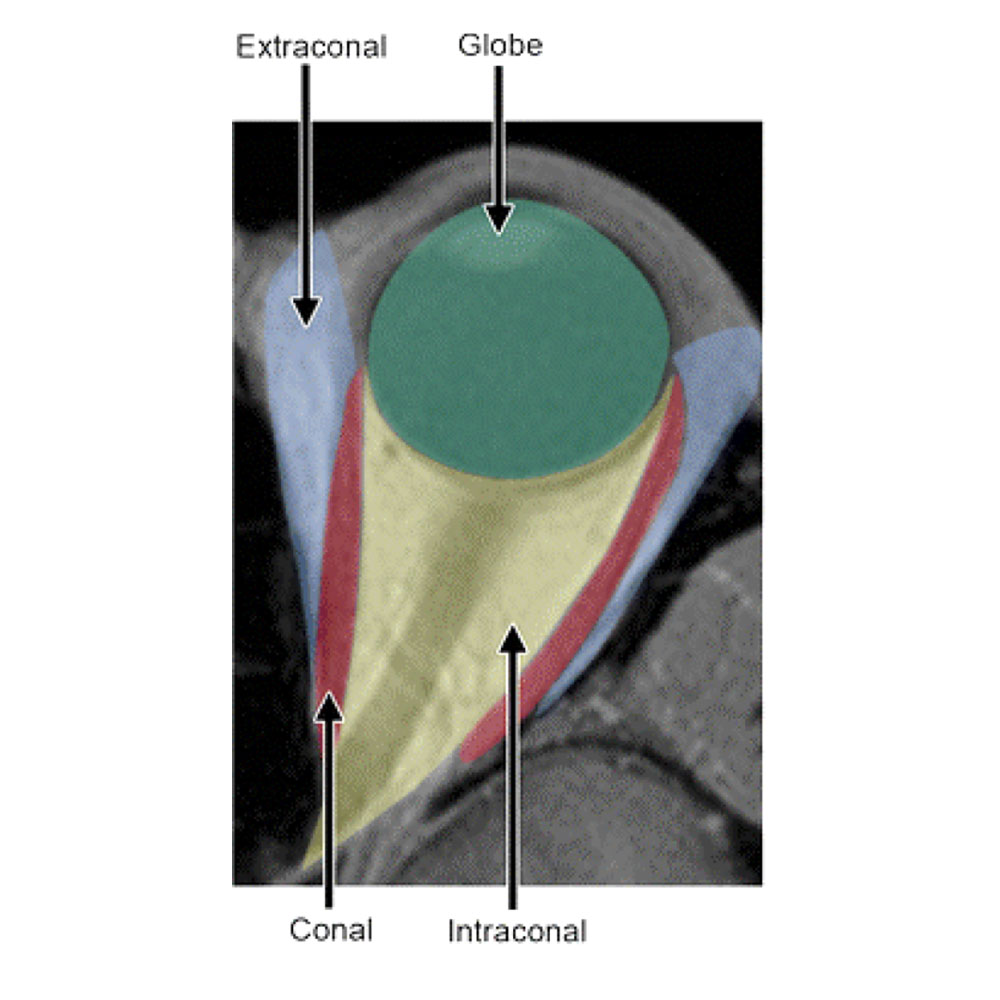
Categorize orbital fat
1.Extraconal fat
The role of extraconal fat is the structure supporting eyeball and muscle cone. So, it is relatively hard and strongly adhering bone, tendon and muscle.
2.Intraconal fat
The role of intraconal fat is the cushioning material for intraconal nerves, vessels during eye movement. It is very soft, loose and indefinite.
To avoid complication
To avoid complication, we should know about those important structure well.
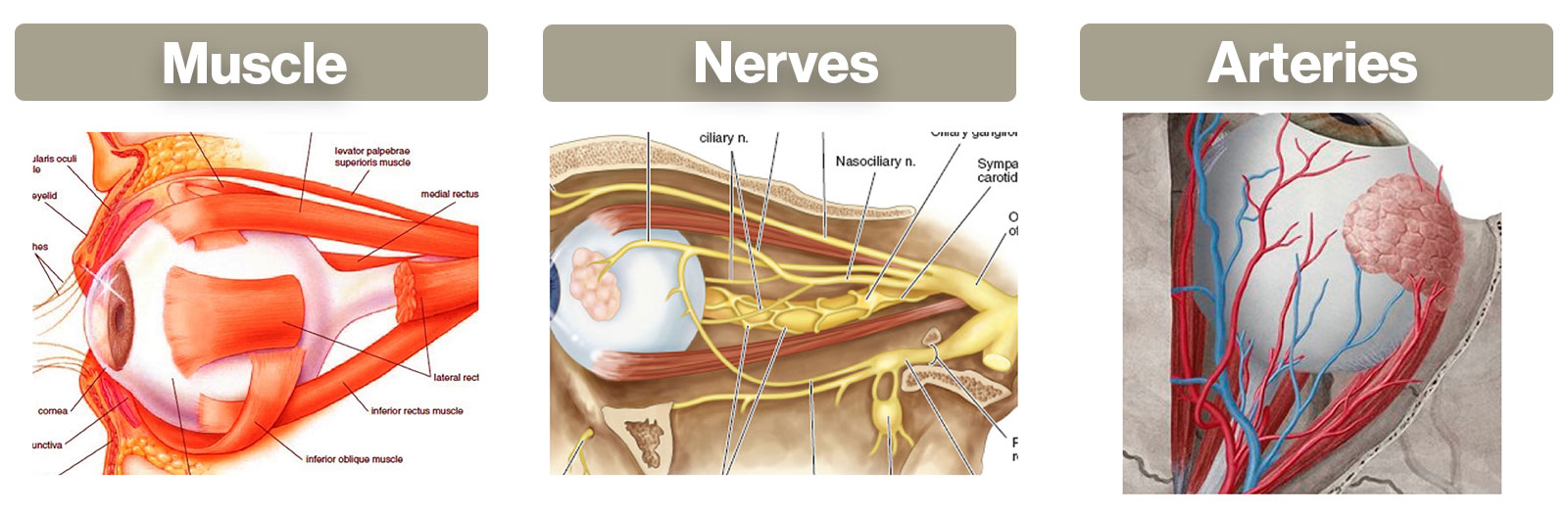
To remove orbital fat, we must consider about muscle, nerves and arteries.
It is not necessary to consider about veins, because rupture of veins never damage visual function.
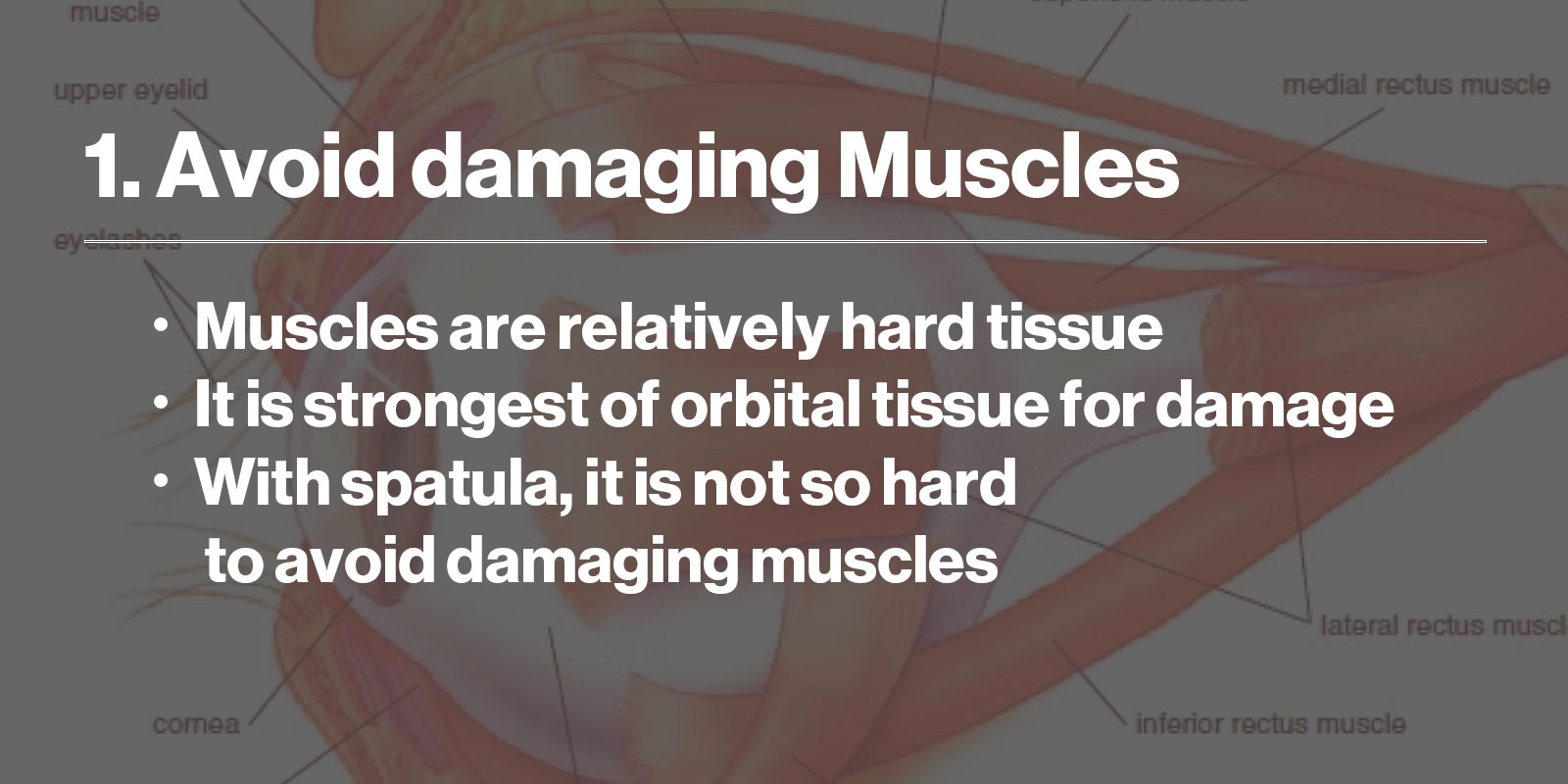
The first, how I avoid damaging muscle?
Muscles are relatively hard tissue. strongest of orbital tissue for damage. With spatula, it is not so hard to avoid damaging muscles.
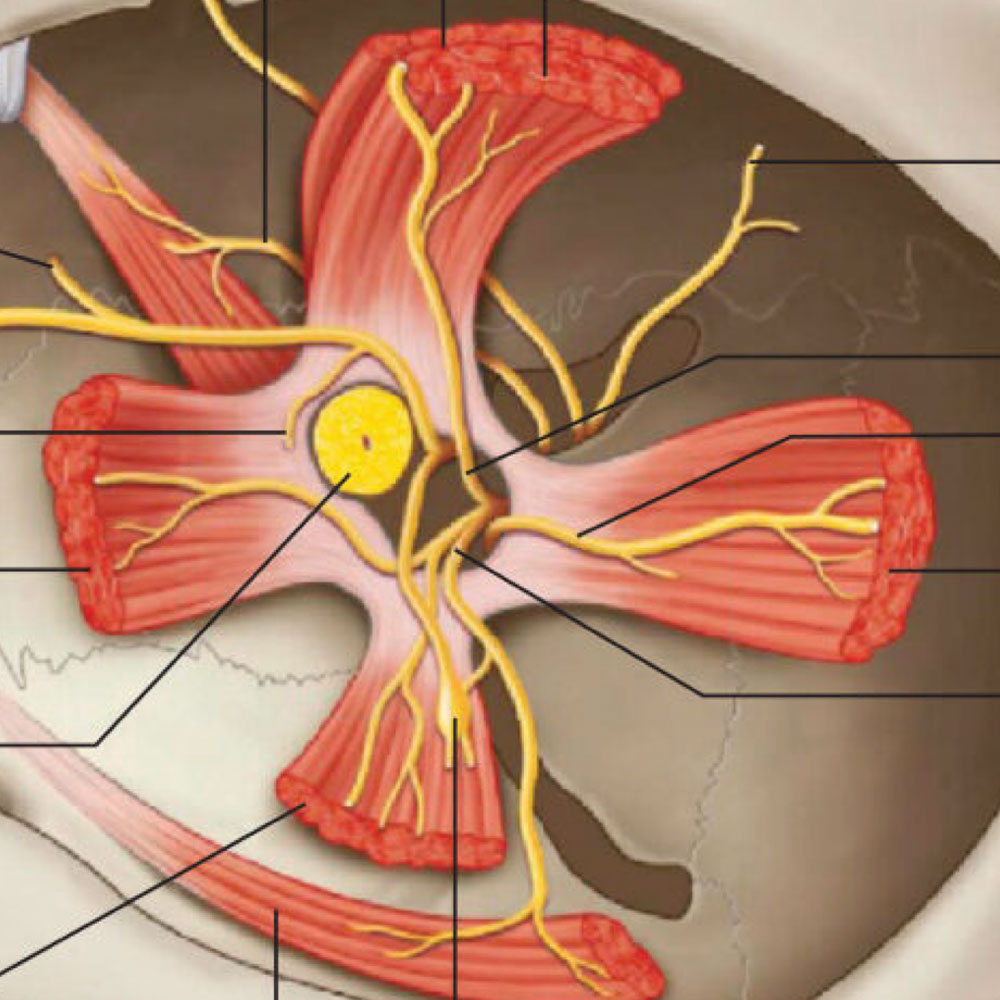
The second, How I avoid damaging nerves?
Optic nerve
Sensory nerve
Motor nerves of extraocular muscles
Short ciliary nerve and ciliary ganglion
We should consider 4 nerves in the orbit. Optic nerve, sensory nerve, motor nerves of extraocular muscles, short ciliary nerve and ciliary ganglion. Needless to say, optic nerve is most important for visual function. Then, damaging the optic nerve is the worst complication.
Because Sensory nerve plays no role for visual function, it is not so important for this surgery. Therefore, during orbital decompression surgery, we must pay attention to those two types of nerves. Motor nerves of extraocular muscles and short ciliary nerve and ciliary ganglion.
motor nerves of extraocular muscles
Distribution of 4 rectus nerve is located optic nerve side of rectus.
Avoid operating the optic nerve side of muscle.
Short posterior ciliary nerve and ciliary ganglion
Intraconal fat is soft, loose and indefinite tissue.
loosen the fat, avoiding tearing off the tiny fibers.
What we should consider to avoid damaging short posterior ciliary nerve and ciliary ganglion.
The intraconal fat is soft, loose and indefinite tissue, so loosen the fat, avoiding tearing off the tiny fibers which may be the branch of oculomotor nerve.
3.Avoid damaging Arteries
Most important tissue for avoiding visual loss is orbital vessels. Because Veins are not important for visual function, I will talk about arteries only.
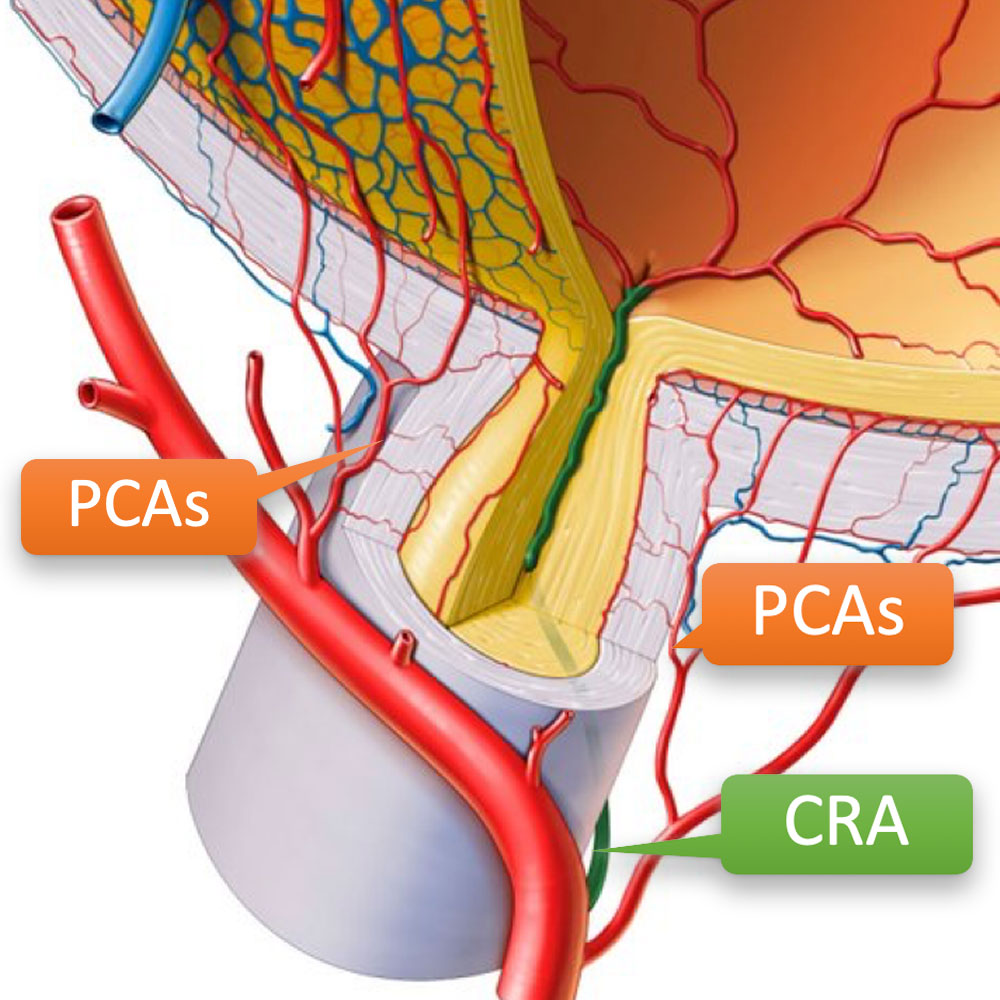
Blood Supply for Vision
We must think about blood supply for eyeball.
Which is more responsible for vision loss after orbital fat decompression? Central Retinal Artery(CRA) or Posterior Ciliary Arteries(PCAs).
Answer: Posterior Ciliary Arteries (PCAs)
Central retinal artery (CRA) is so close to optic nerve that CRA rupture is possible but rare.
Rupture of PCAs is more probable. It must cause Anterior Ischemic Optic Neuropathy(AION).
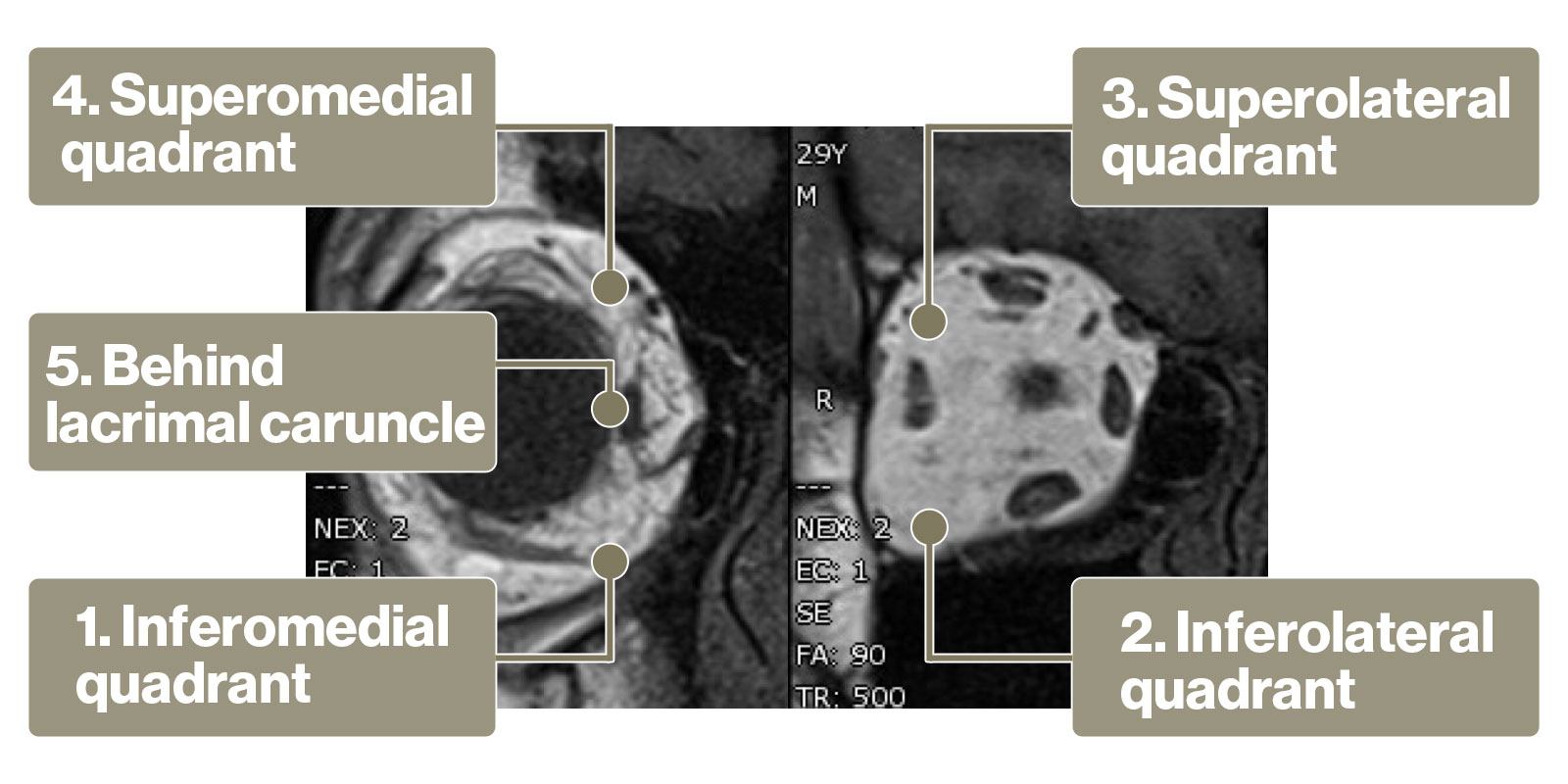
Which area of orbital fat can be removed?
Then, which area of orbital fat can be removed?
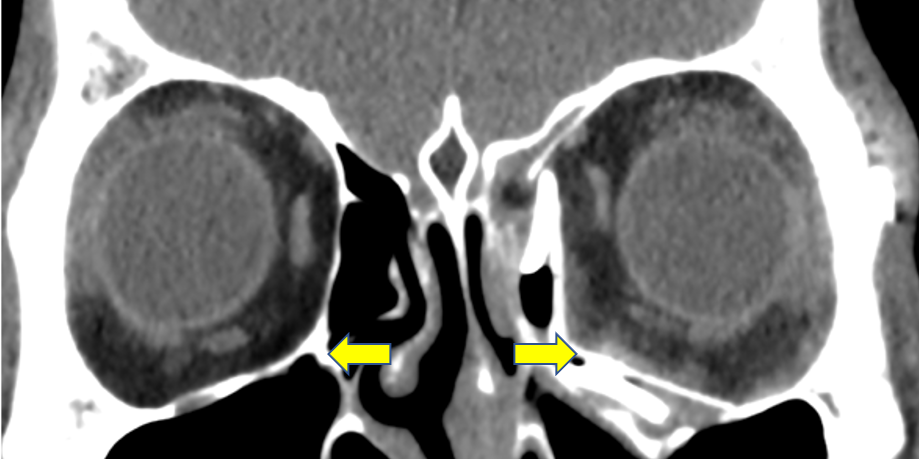
This MRI can is from the patient of thyroid eye disease.
So, which area of fat do you think be removed?
Fat removal from 4 quadrant
Of course, Orbital fat can be removed from 4 quadrant avoiding 4 rectus muscles.
And last, just behind lacrimal caruncle.
Orbital fat of lower quadrant can be removed from inferior fornix and upper quadrant can be removed from upper eyelid crease.
Schema of orbit
1. Removing fat must be posterior to equatorial part of eyeball.
2. The more posterior you go, the more effective it is.
Now I explain the basic concept of orbital fat decompression. The first, removing fat must be posterior to equatorial part of eyeball. Anterior part of orbital fat play no role for protrusion.
The second, The more posterior you go, the more effective it is. The cross-sectional area of orbit changes depending on the position. So, posterior fat removal is more effective, but it is also dangerous.
How I remove it?
1.Extraconal fat
You can just remove it roughly under adequate knowledge of orbital anatomy.
2.Intraconal fat
You must remove intraconal fat gently. Using 2 spatula, push aside 2 rectus muscles for each quadrant, then intraconal fat will pop out from the intermuscular septum.
The fat should be loosened before removing. And only loosened fat can be removed. Intraconal fat contains tiny but important nerves and arteries.
You must pay maximum attention for removing.
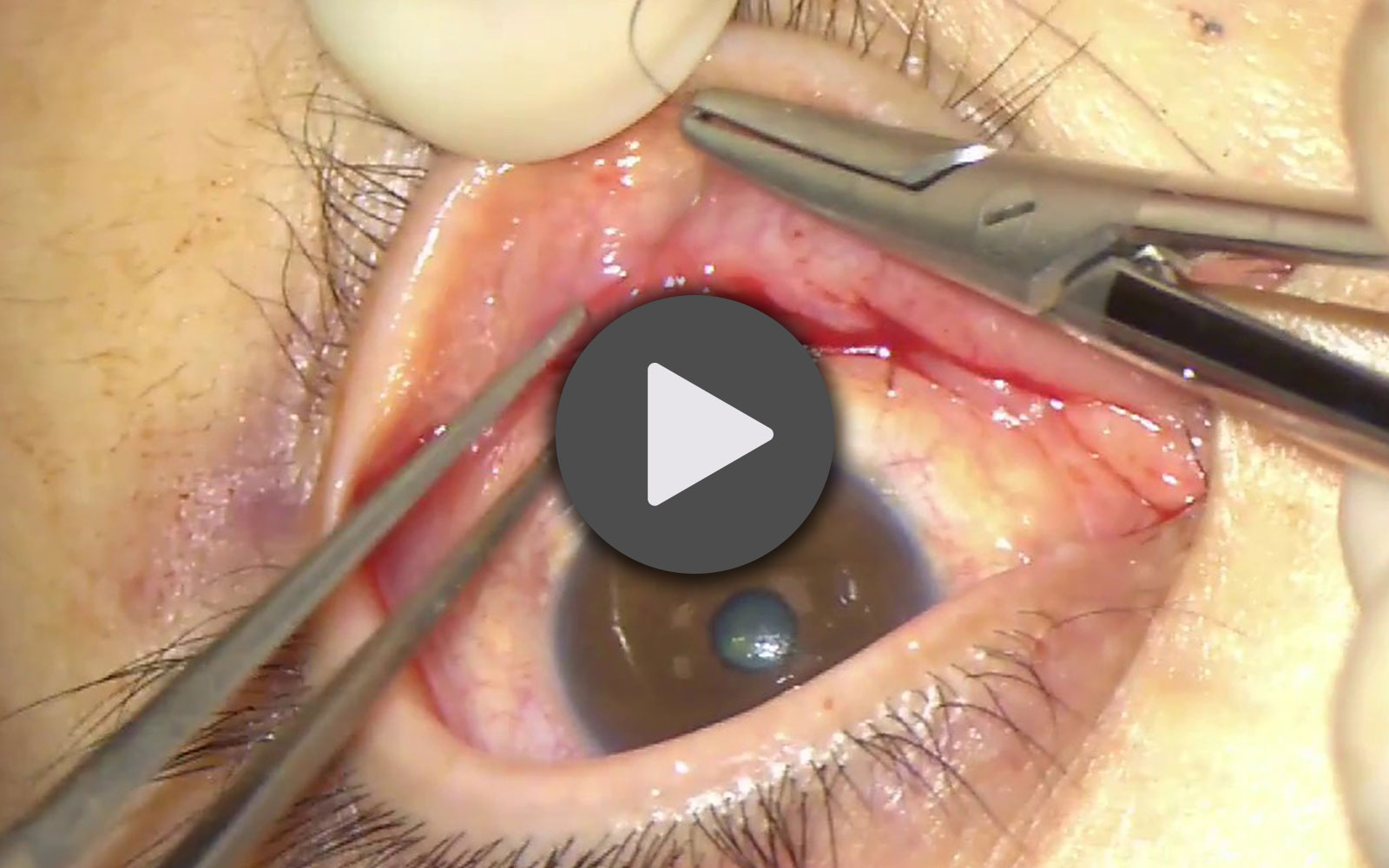
Intraconal and Extraconal Fat decompression fornix approach
This is the movie of fat decompression. You can see this video in my youtube channel.
With the transconjunctival approach, fat tissue can be removed. At first, we remove blepharoplasty fat, and extraconal fat.
Then we remove intraconal fat from the space of muscles, between inferior rectus and lateral rectus, and between inferior rectus and medial rectus.
CASES
30 years old Female
Pre
She has fatty hyperplasia of both upper and lower eyelids with ocular protrusion.
Post
Both upper and lower eyelids show improvement in adipogenesis.There seem to be no fat gain due to thyroid eye disease.
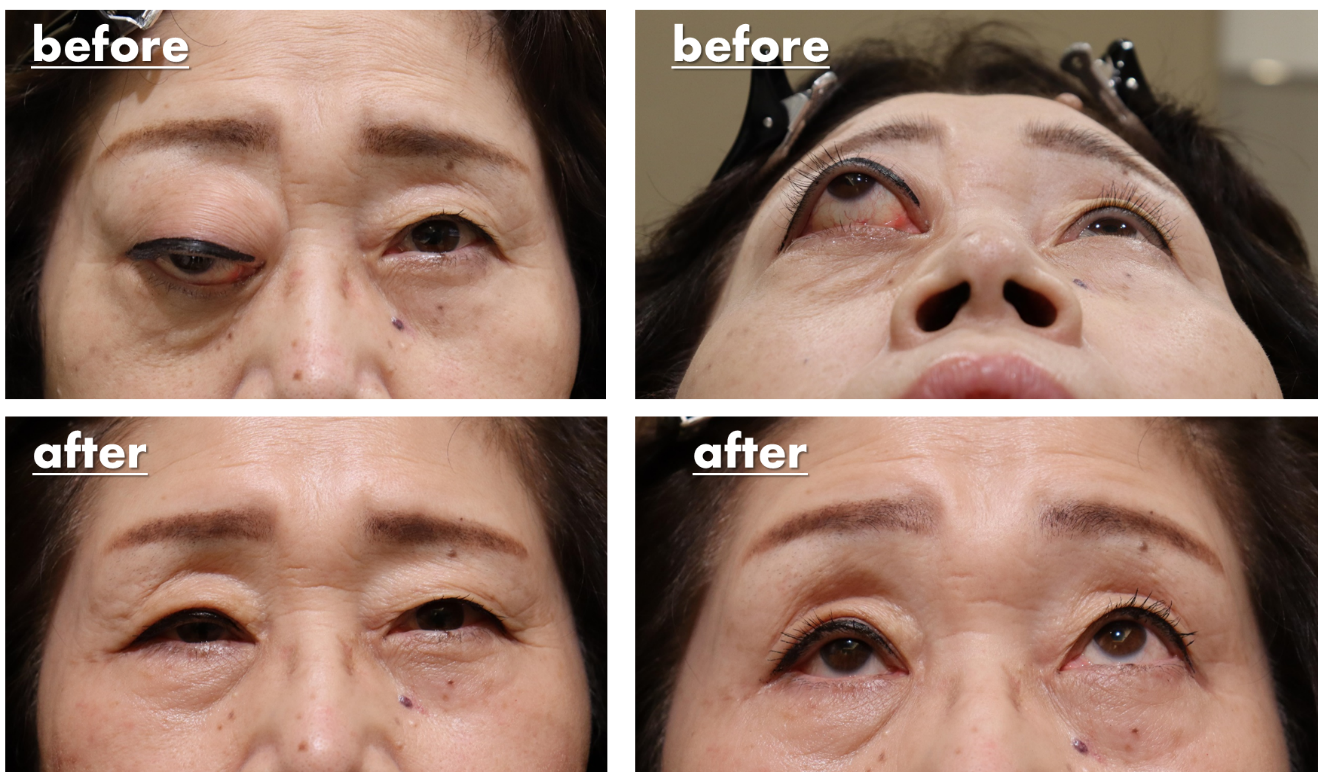
40 years old Female
This is the result after fat decompression. We performed both upper and lower fat decompression for this case.
Pre
Before surgery, upper and lower eyelid was puffy and swollen.
Post
After surgery, the eyelid become thin, skinny.Especially, please check far side of upper eyelid, eyelid become sharp and natural.
30 years old Female
Pre
After onset of thyroid eye disease, her appearance has completely changed.
Post
After two types of fat decompression, she was back to her old self.Thyroid eye disease make both eyes apart, Removing fat of just behind the lacrimal caruncle, where is medial position of eyeball, eyes become closer.
For congenital enophthalmos
Case1.30 years old Male
Orbital fat decompression can treat congenitally proptotic patient.
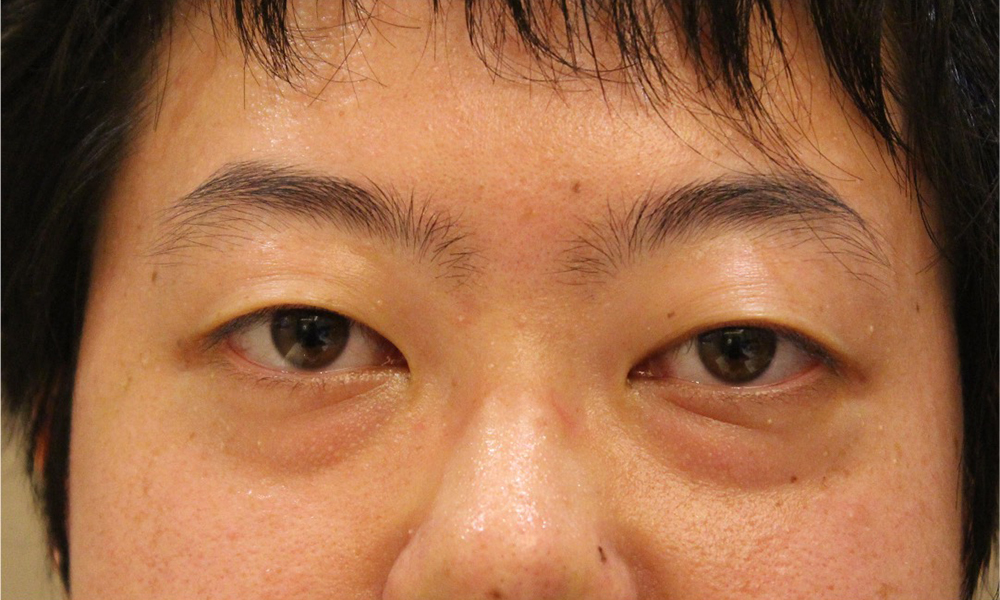
Pre
Her eyes bulge out, her upper eyelids bulge, and her lower eyelids have dark circles.
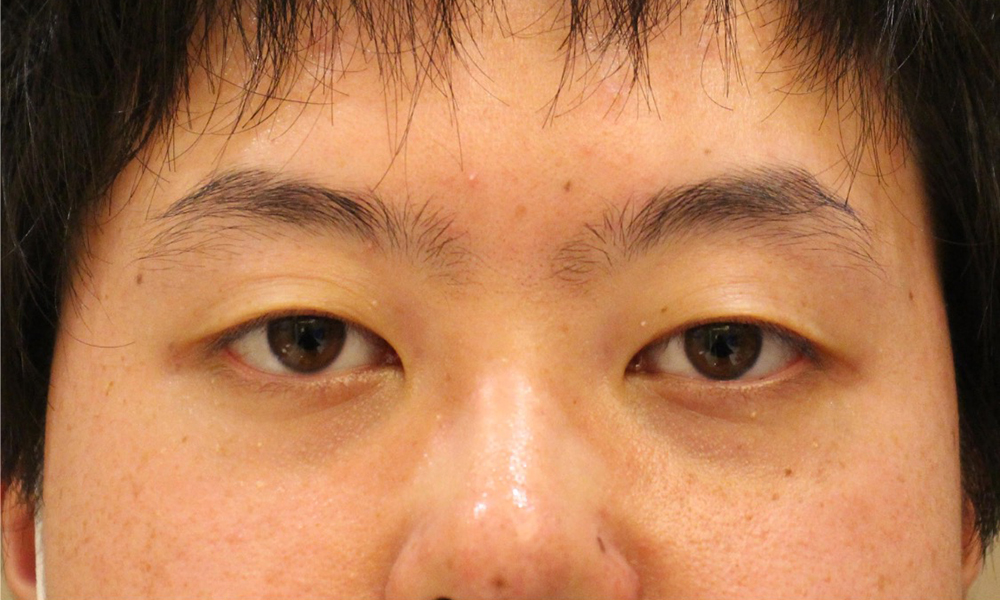
Post
Eyes are smaller, upper eyelid bulge and lower eyelid dark circles have improved.
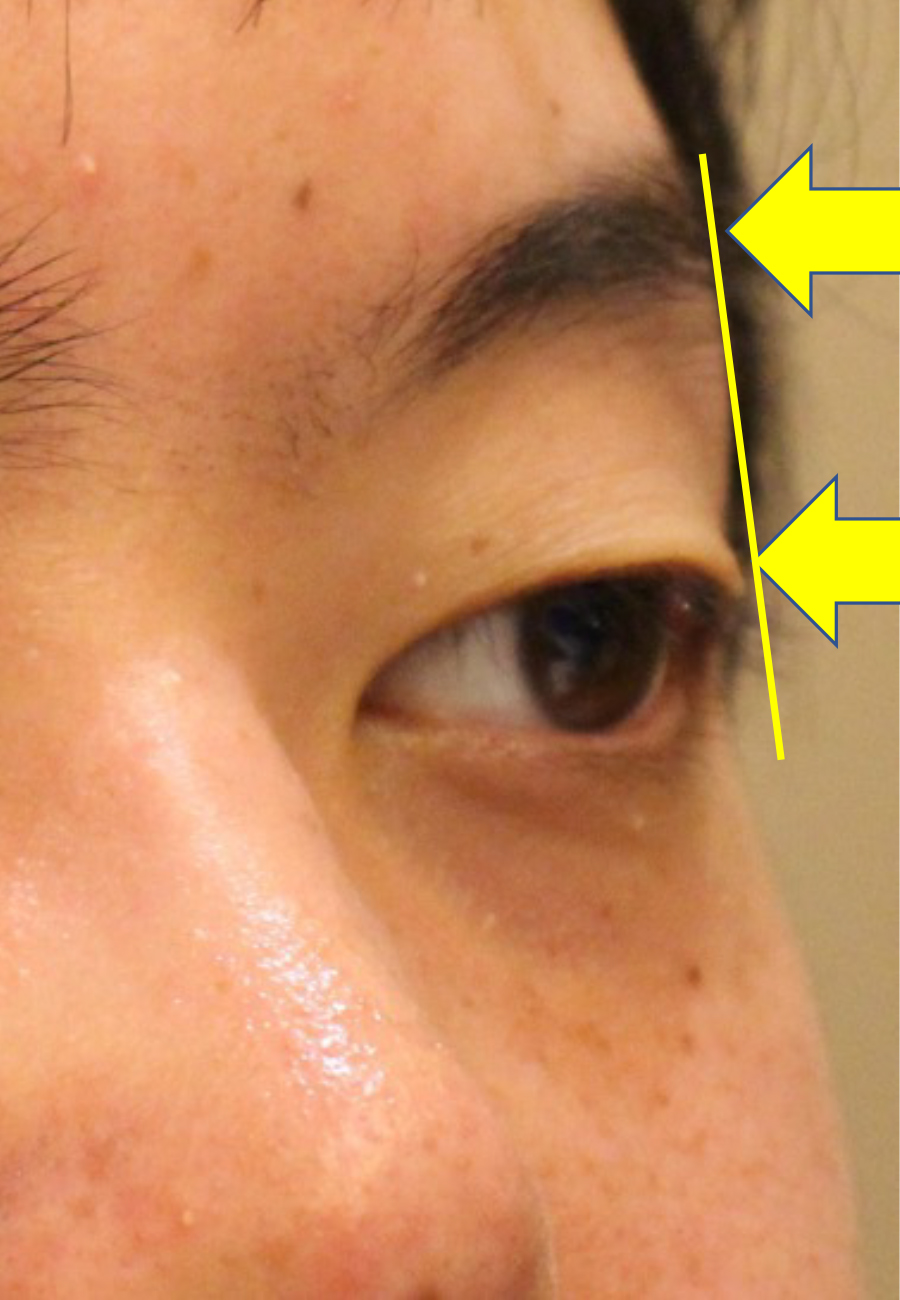
However, from the side, you can understand the change.
Comparing the top of eyelid and eyebrow, it is remarkable eyeball position changed
Different from thyroid eye disease, congenital proptosis do not have increasing volume of fat.
So there is limitation to remove the fat.
Pre
The upper eyelids are swollen and the lower eyelids have dark circles.
Post
Eyes are smaller, upper eyelid bulge and lower eyelid dark circles have improved.
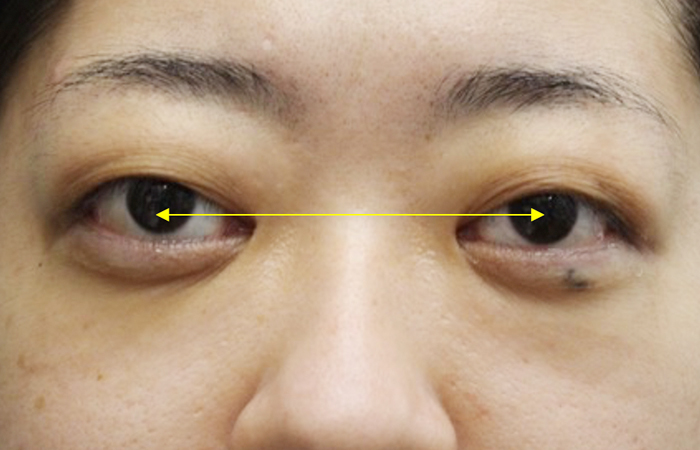
Case2.Explaining orbital decompression using case photos
Compare photos before and after treatment
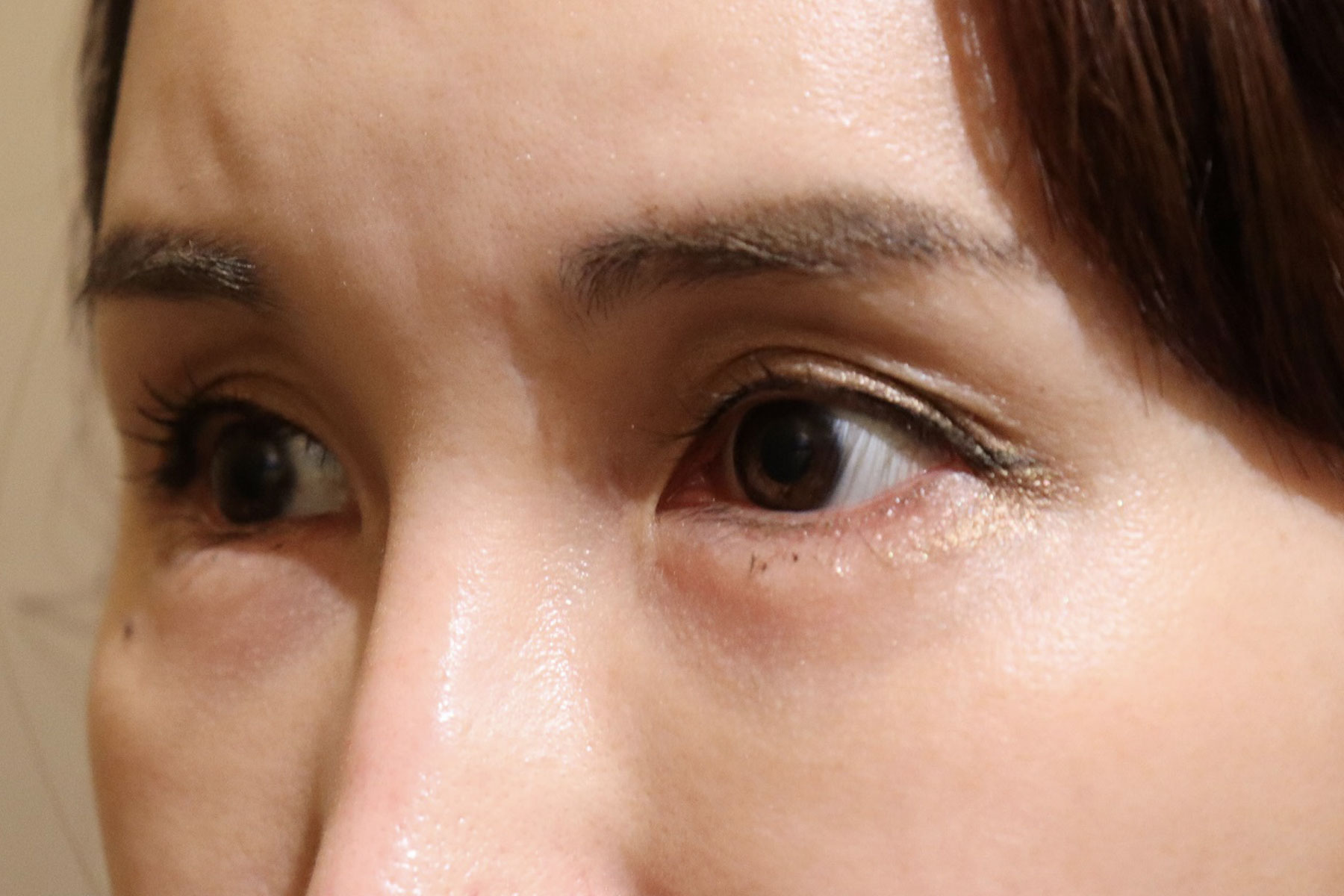
Please take a look at the pre-surgery photos. She has beautiful eyes with double eyelids, but the whites of her eyes are exposed a lot, and her upper eyelids look a little swollen, so she came to our clinic hoping to have these things corrected.
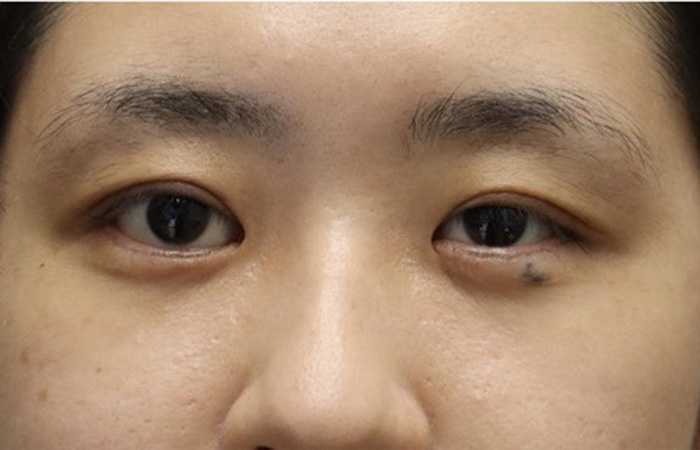
Next, please take a look at the photos taken 1 month after surgery.
There are still traces of bleeding on the lower eyelids and whites of the eyes. It usually takes 3-4 weeks for the bleeding to subside. You can see that the sunken eyes give a gentler impression.
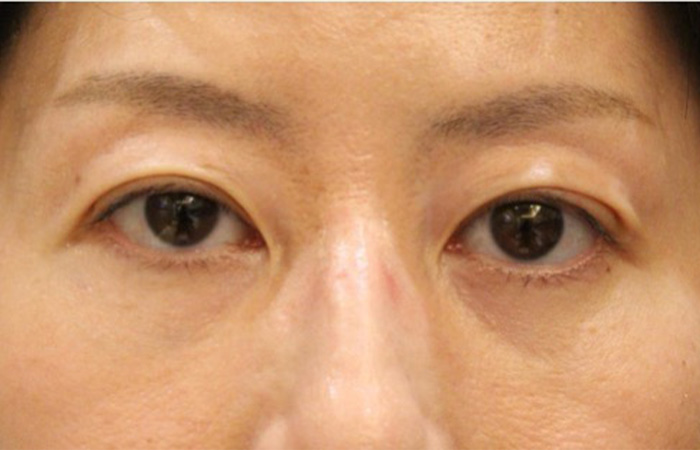
Easy to understand and enlarge
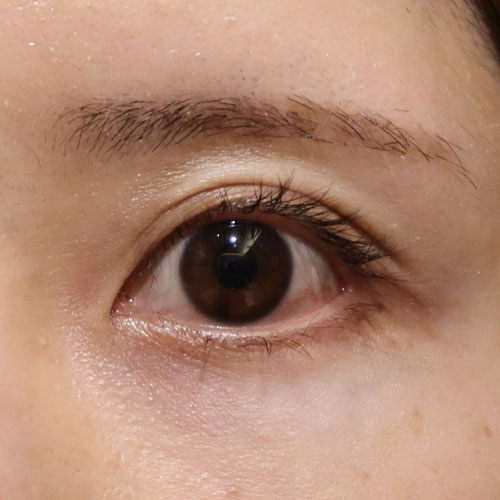
Pre
There is a bulge in the upper eyelids, giving the impression of being a little chubby. The area of the whites of the eyes is also large.
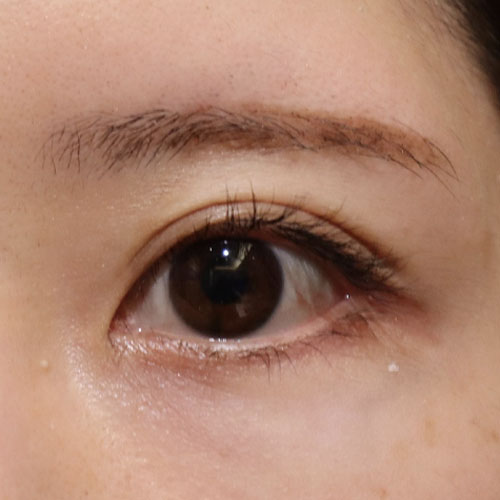
Post
It’s been 2 weeks since the fat was removed from the lower eyelid and behind the eyeball. I still have bleeding in the whites of my eyes and lower eyelids. The area of the whites of the eyes has decreased. Also, because the eyes are sunken, both the upper and lower eyelids cover the eyes, reducing the exposure of brown eyes.
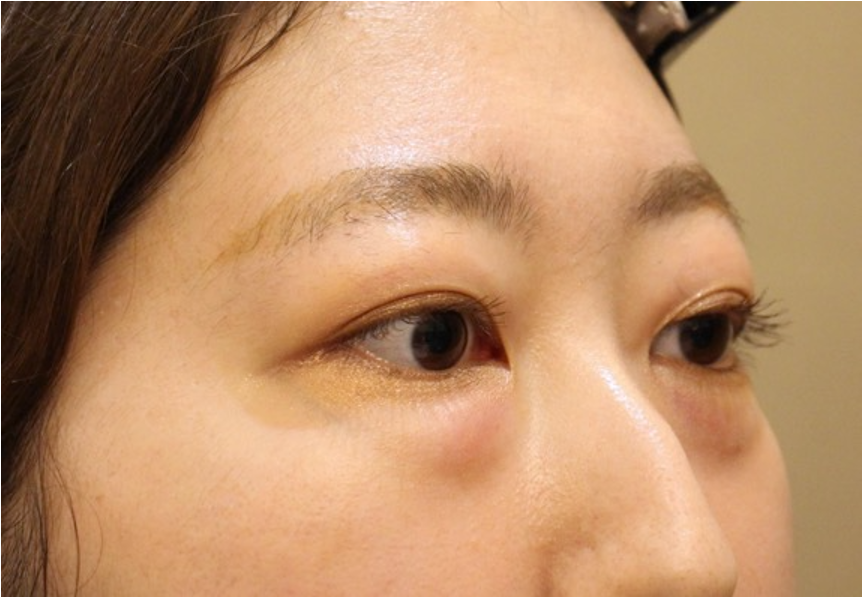
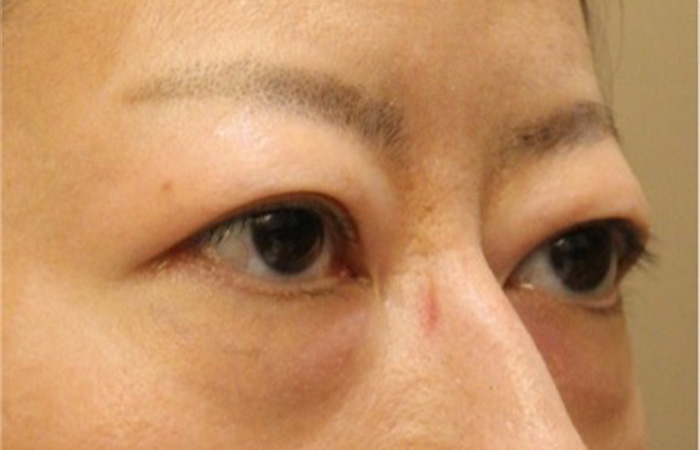
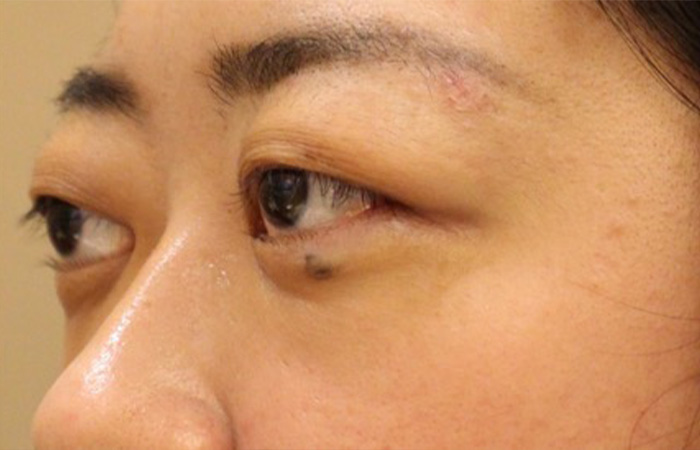
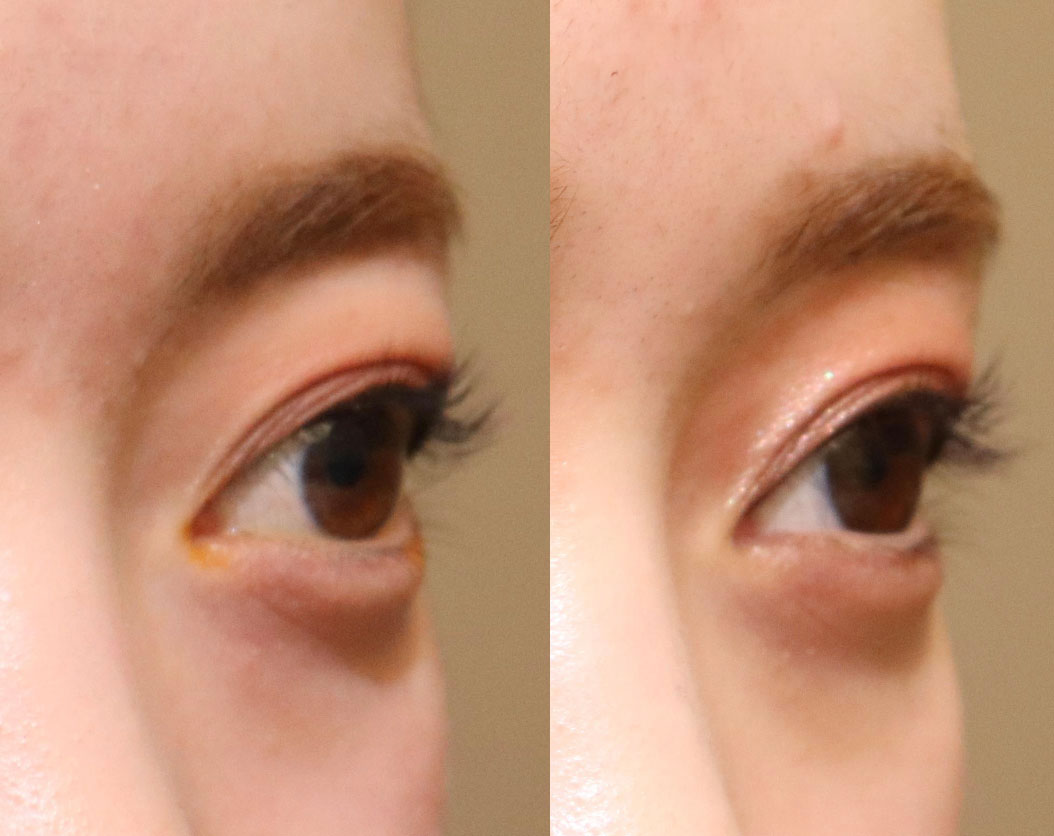
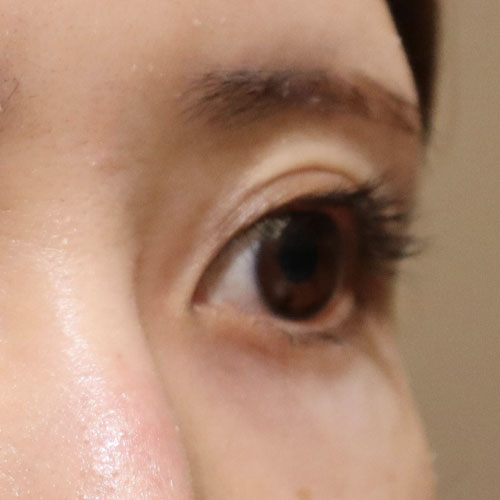
Next is a photo taken from an angle.
Pre
She has beautiful eyes with double eyelids, but the whites of her eyes are exposed a lot, and her upper eyelids have a slightly swollen shape.
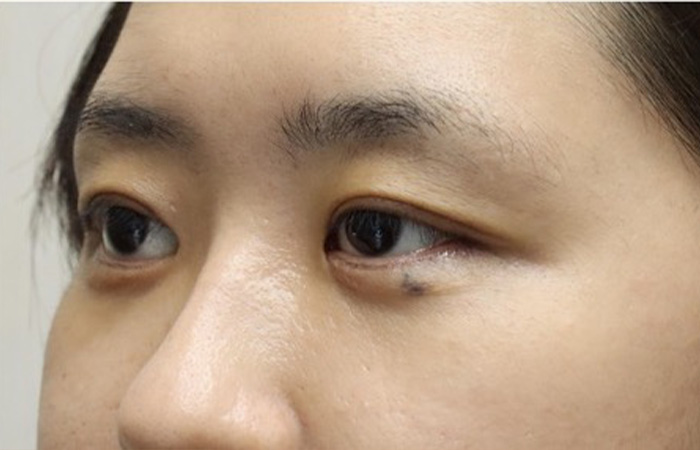
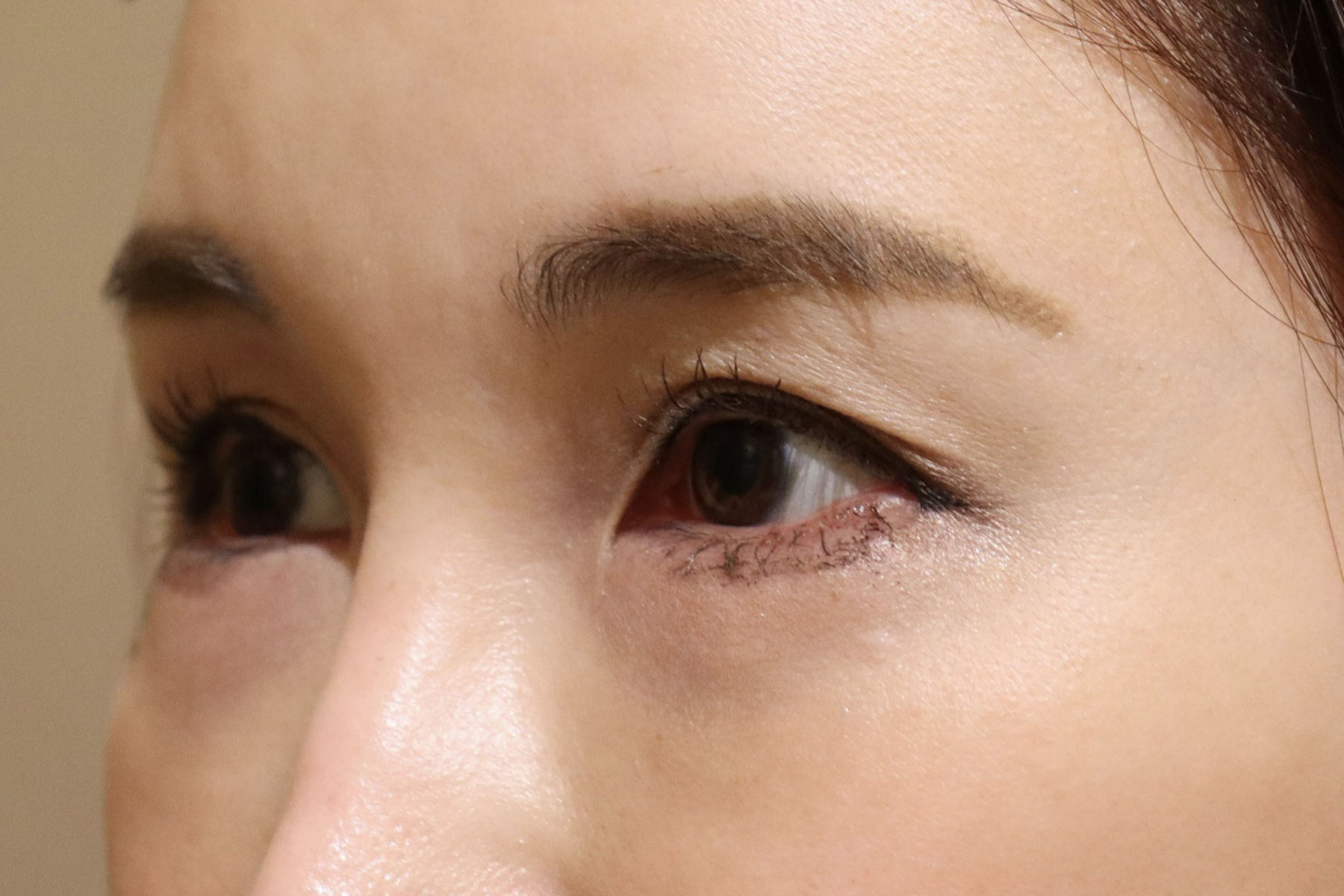
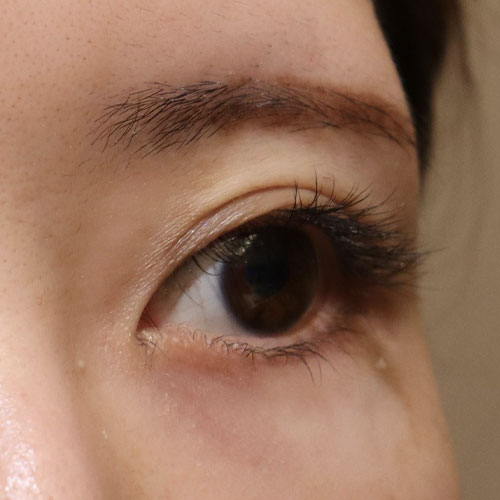
Post
Comparing the area of the whites of the eyes, the area of the whites of the eyes is smaller after surgery. Her eyes are a little smaller, giving her a more beautiful look. My upper eyelids also feel refreshed.
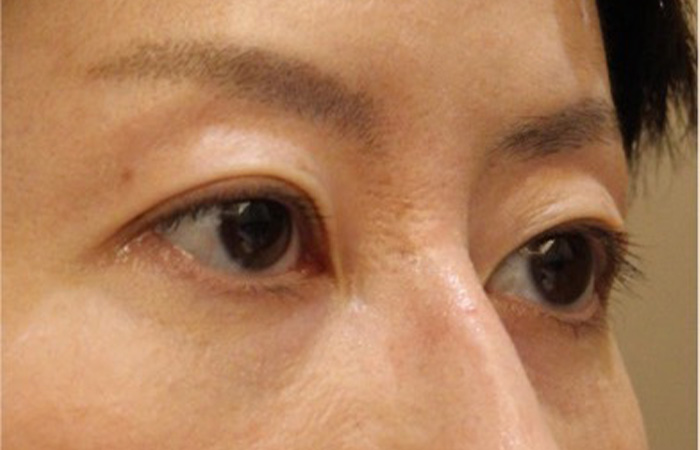
Please pay attention to your left eye
Compare photos before and after treatment
Comparing the left upper eyelid in an oblique photo, you can see that the puffiness has disappeared and the upper eyelid, which used to protrude more than the eyebrows, has become more depressed than the eyebrows after surgery.
In this way, you are born with large eyes (protruding eyes), and our clinic also performs corrections for this. If you have a similar problem, please feel free to contact us.
Risk
Risk of complications
Bleeding, infection, double vision, visual field disturbance, visual impairment, general anesthesia
Cases of congenital bulging eyes
Case3.If the patient need to remove fat more…
Explaining a case of congenital exophthalmia
Deepening of orbital sulcus cause completely different appearance which may bring impression of aged person.
Compare photos before and after treatment
Pre
The eyes are large and give the impression that they stand out too much. The area of the whites of the eyes is large, making them look like Sanpaku eyes. It also looks like the eyes are a little far apart.
Post
This is a photo taken the day after surgery. You can see that the eyes are sunken and the area of the whites of the eyes has decreased. The distance between my eyes has become closer and my balance has improved. The black lower eyelid is due to internal bleeding.
Easy to understand and enlarge
Pre
I have enlarged the photo for clarity. The area of the white of the eye is large, and there is also the white of the eye between the cornea and lower eyelid.
Post
This is a photo taken the day after surgery. You can see that the upper eyelids are sunken and the area of the whites of the eyes is reduced. The white of the eye between the lower eyelid and cornea is gone, and the tripaku has resolved. The black lower eyelid is due to internal bleeding.
Next, let’s take a look at the photo from an angle.
Pre
It is noticeable that the eyes are very large. I think people with small eyes would be envious of them, but having them too big can also be a problem.
Post
In the photo taken the day after surgery, the area of the whites of the eyes has decreased and the impression that the eyes are large no longer appears. It has changed to a calmer impression.
Enlarge the photo of the right eye
Again, we may remove fat as much as possible if patient demands, but it may result worsening of impression.
Pre
The position of the eyebrows and the position of the eyeballs are approximately the same height.
Post
It’s the day after surgery. As the eyeballs become sunken, the upper eyelids become sunken, and as a result, the area of the whites of the eyes becomes smaller.
Case4.40 years old male
Pre
The eyes are bulging and the upper eyelids are bulging.
Post
His eyes became sunken and small. The swelling of the upper eyelids was reduced.
Conclusion
As a conclusion, any exophthalmos can be treated by orbital fat decompression surgery to some extent.
Orbital tumor resection
The two main approaches to the ORBIT are
Transcutaneous approach
Transconjunctival approach
I prefer transconjunctival approach for aesthetic reason.
About the extraorbital approach
The approach to the orbit began with avoiding intraorbital injury leading to loss of visual function.
However, the extraorbital approach is highly invasive.
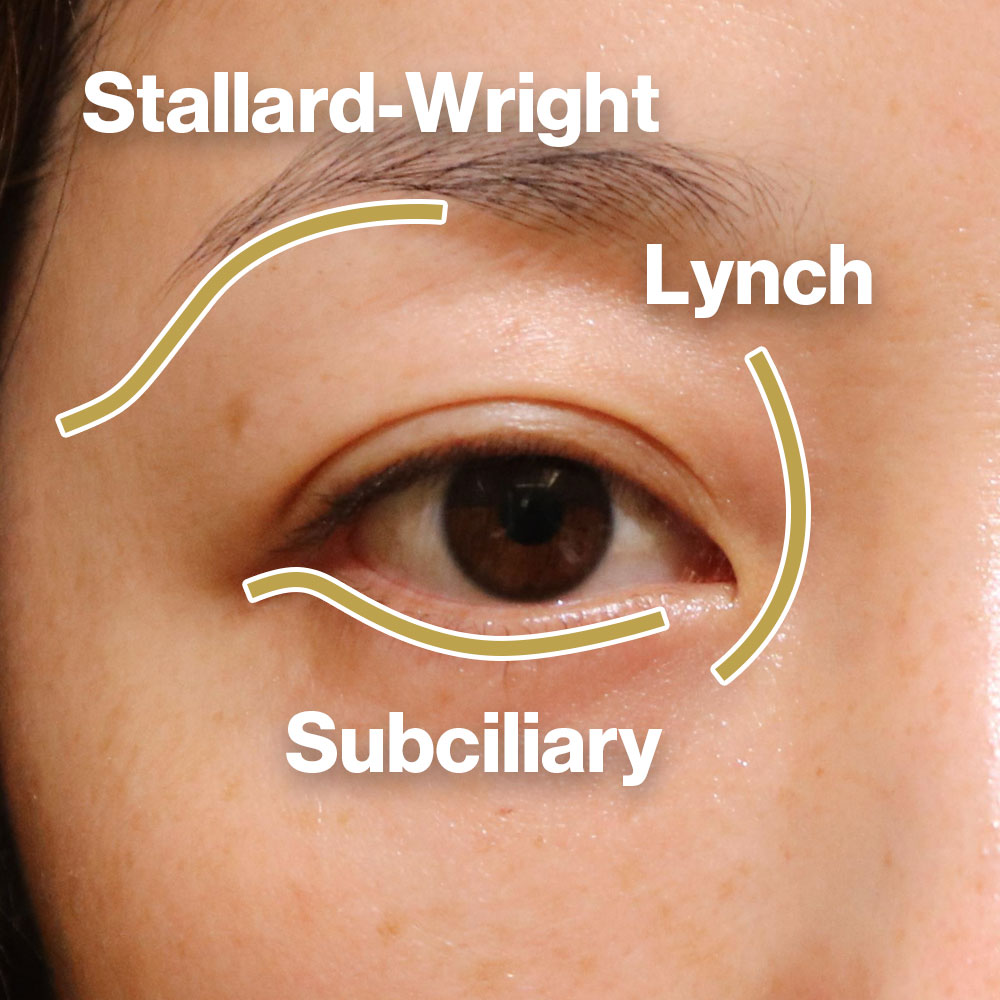
10 approaches to the orbit
This is an illustration from the American Academy of Ophthalmology.
Many approaches have been developed and there are more than 10 approaches as shown here.
A. Classic Stallard-Wright lateral orbitotomy.
B. Eyelid crease lateral orbitotomy.
C. Lateral canthotomy/ cantholysis orbitotomy.
D. Transcaruncular medial orbitotomy.
E. Frontoethmoidal (Lynch) medial orbitotomy.
F. Upper eyelid crease anterior orbitotomy.
G. Vertical eyelid split superomedial orbitotomy.
H. Medial bulbar conjunctival orbitotomy.
I. Subciliary inferior orbitotomy.
J. Transconjunctival inferior orbitotomy.
K. Lateral bulbar conjunctival orbitotomy.
Different approaches are used depending on the location of the tumor in the orbit.
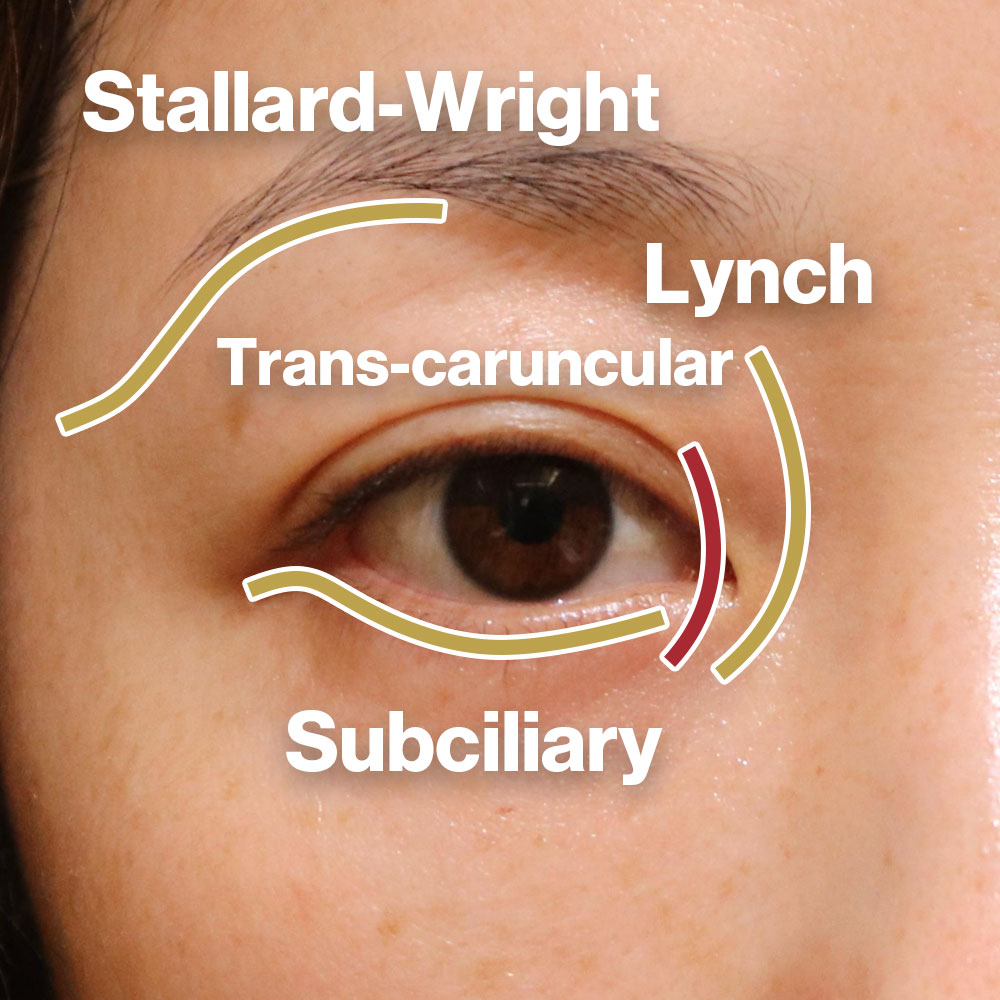
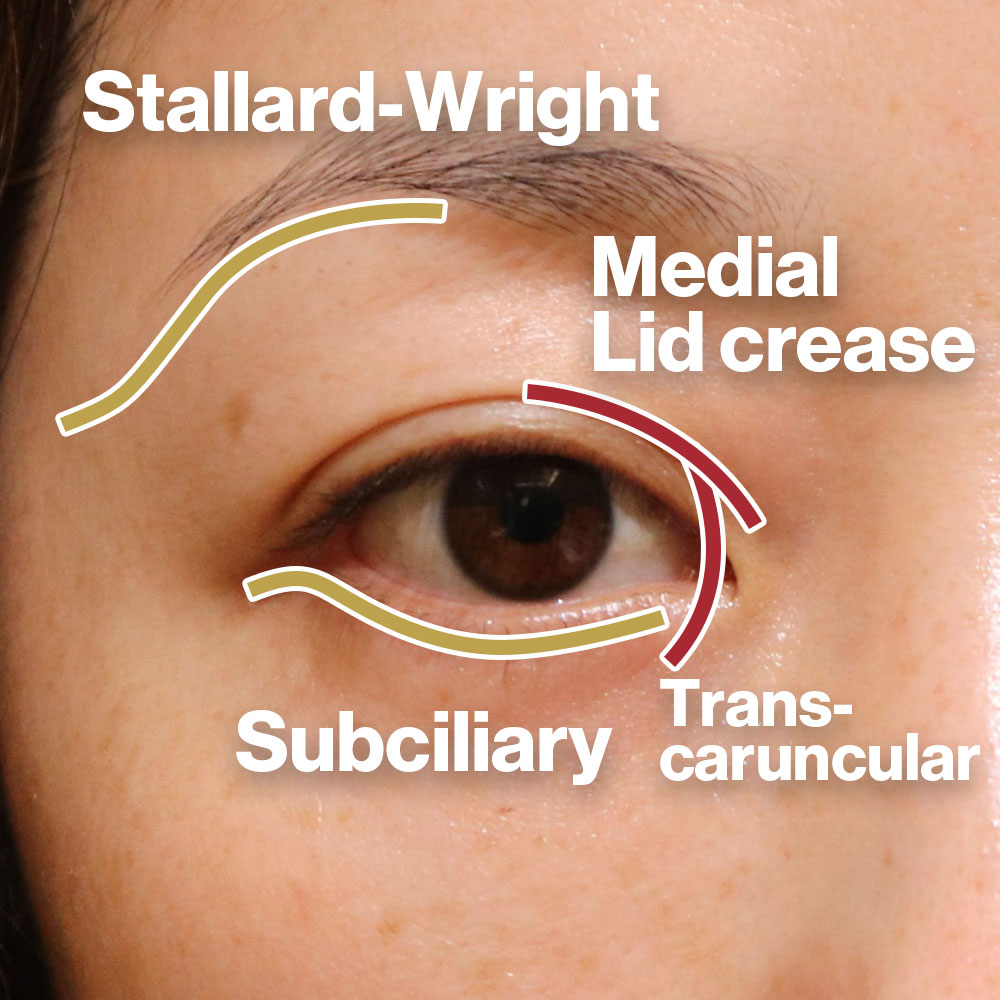
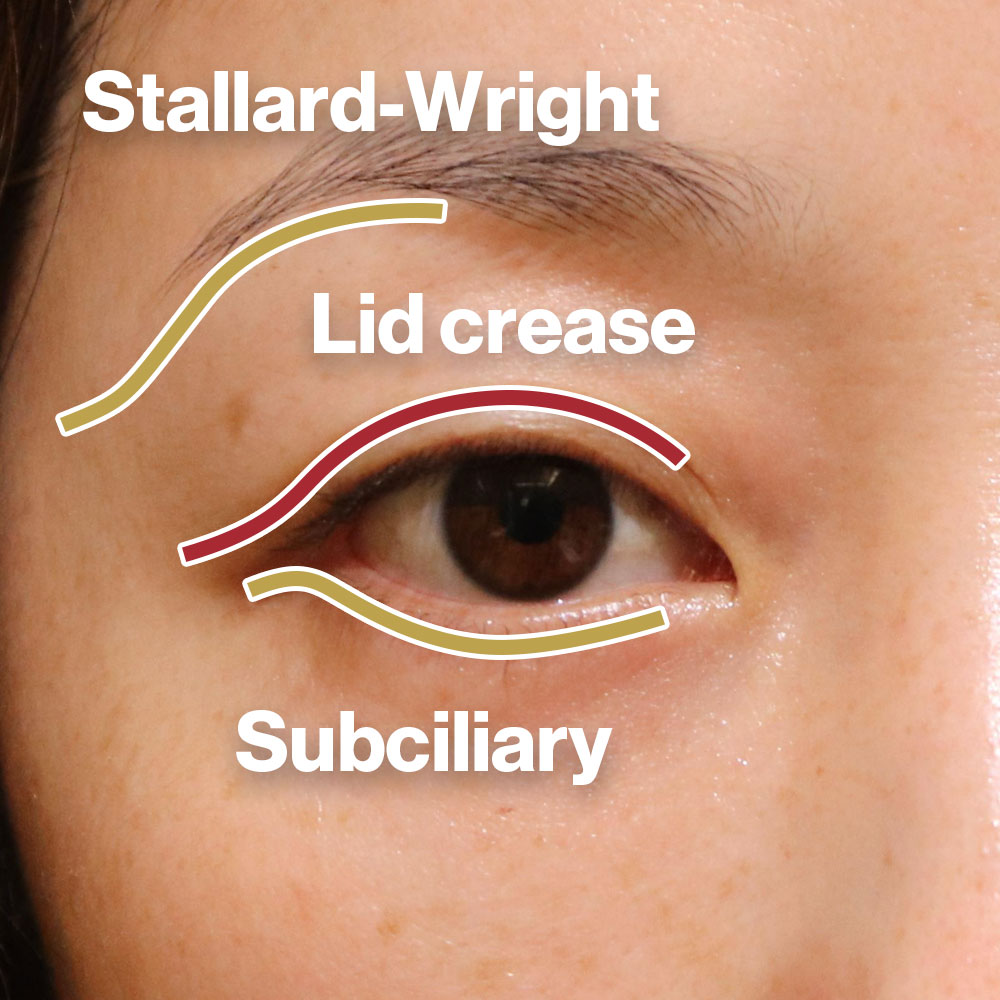
Minimally invasive as technology advances
This is the classic transcutaneous approach that has been practiced for decades.
This approach leaves a scar formation on the skin, is far from the orbit, and is highly invasive, so it is gradually being phased out in modern times.
The Lynch incision approach has been replaced by the less invasive trans-caruncular approach.
If the approach is superomedial, lid crease incision approach is also possible.
The superolateral orbital approach has shifted to an approach from the lid crease incision approach.
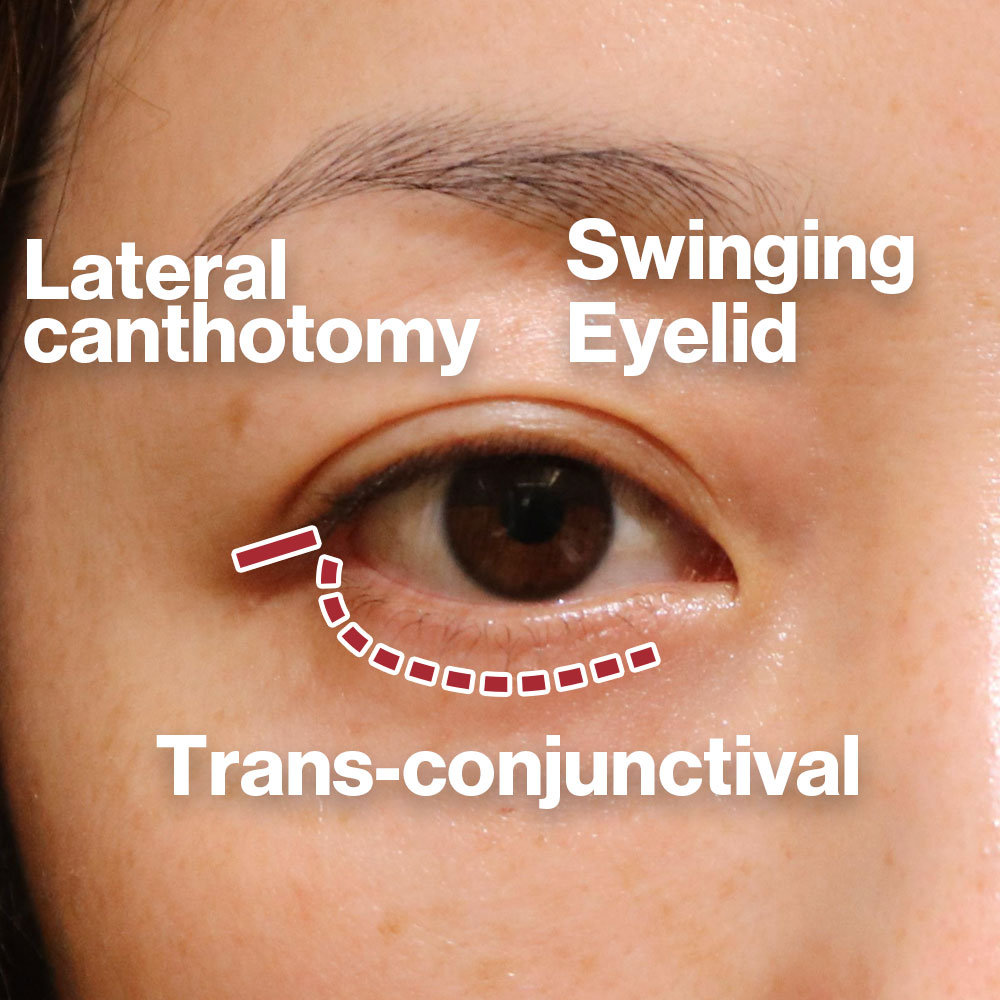
The subciliary approach is shifting to conjunctival incisions, lateral canthotomy incision, or a combination of both called swinging eyelid approach.
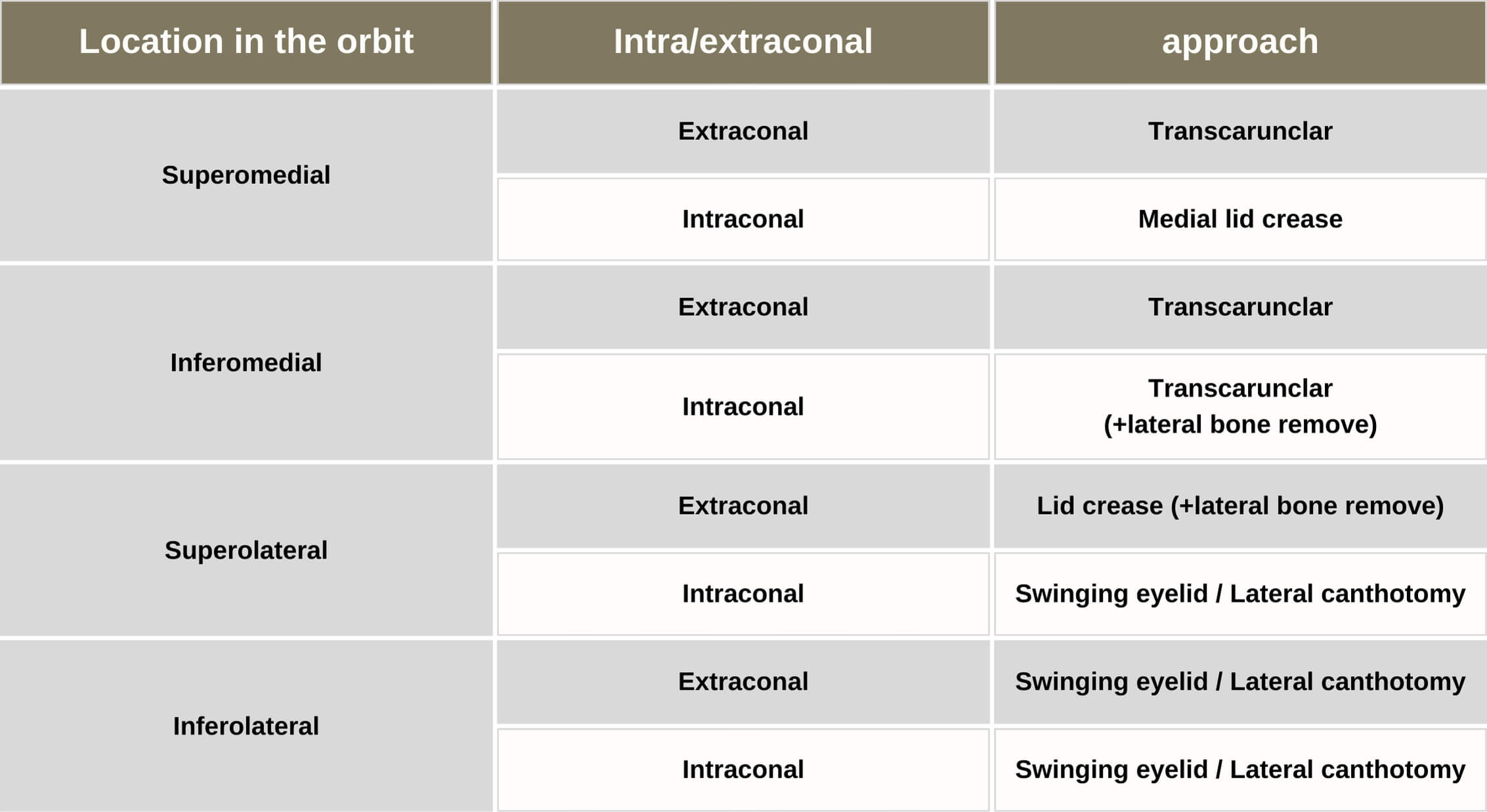
This is a list of my preferred approaches.
I vary my approach depending on where in the orbit the tumor is located.
Specifically, the approach I choose depends on where in the four quadrants of the orbit and whether it is Extraconal or Intraconal.
The Lateral canthotomy approach
Now, I would like to move on to each of the topics.
First, the Lateral canthotomy approach.
Orbital tumor
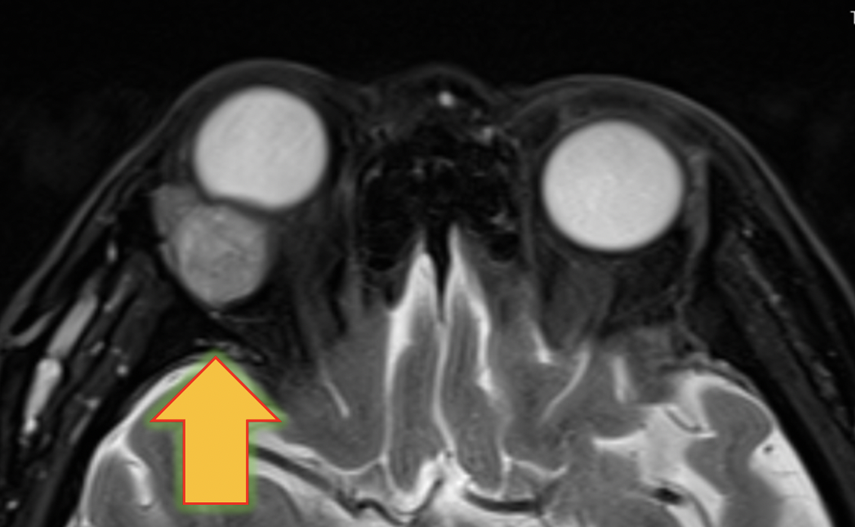
70 years old Female
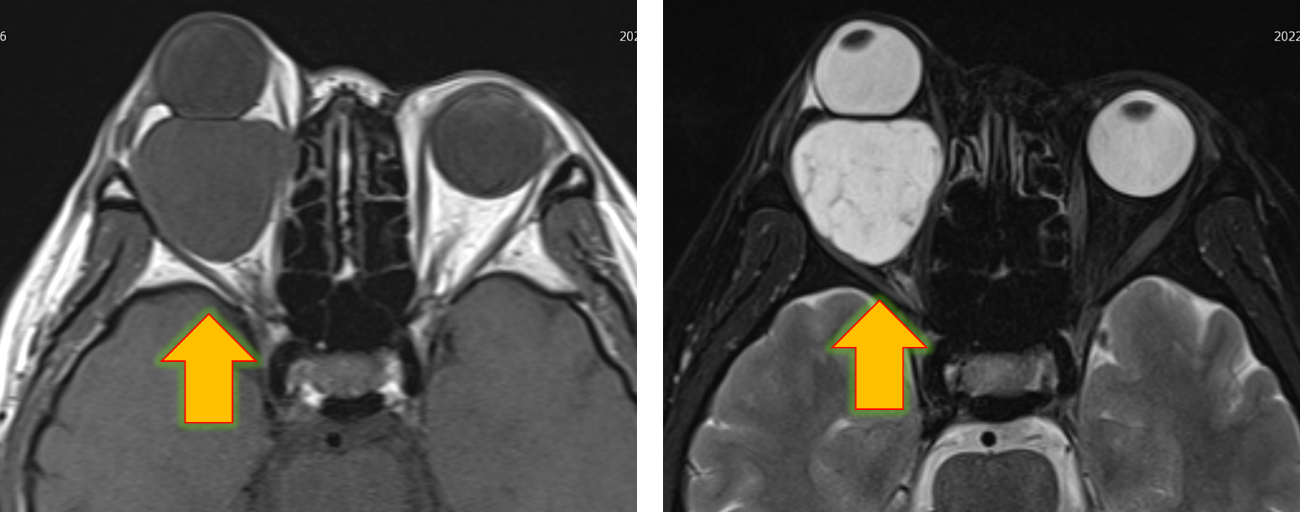
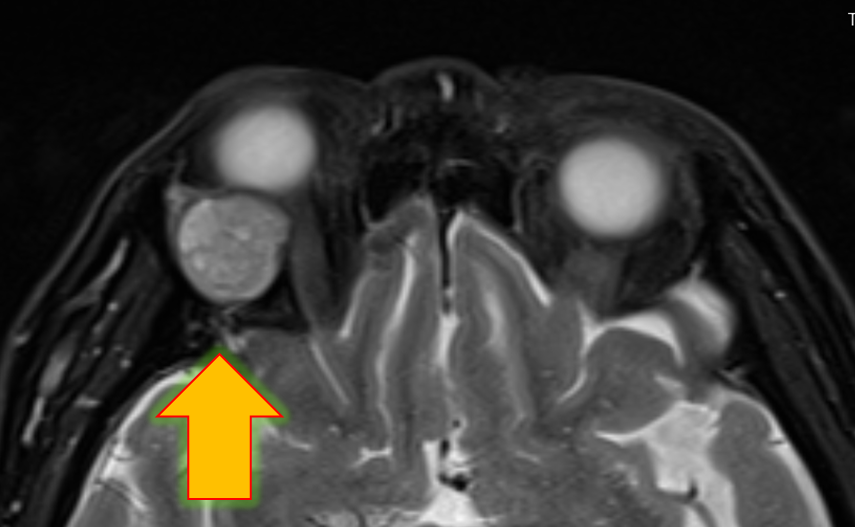
Right huge intraconal orbital tumor
Operation refused by neurosurgeon
This patient is approximately 70-year-old woman. She had been seeing a neurosurgeon, but because there’s a risk of blindness, she has not been able to undergo surgery until now. Gradually, the protrusion of right began to interfere with daily life, not only in terms of function but also in terms of appearance. She came to our hospital looking for a medical institution that could treat her right eye
Intraconal tumor bigger than eyeball
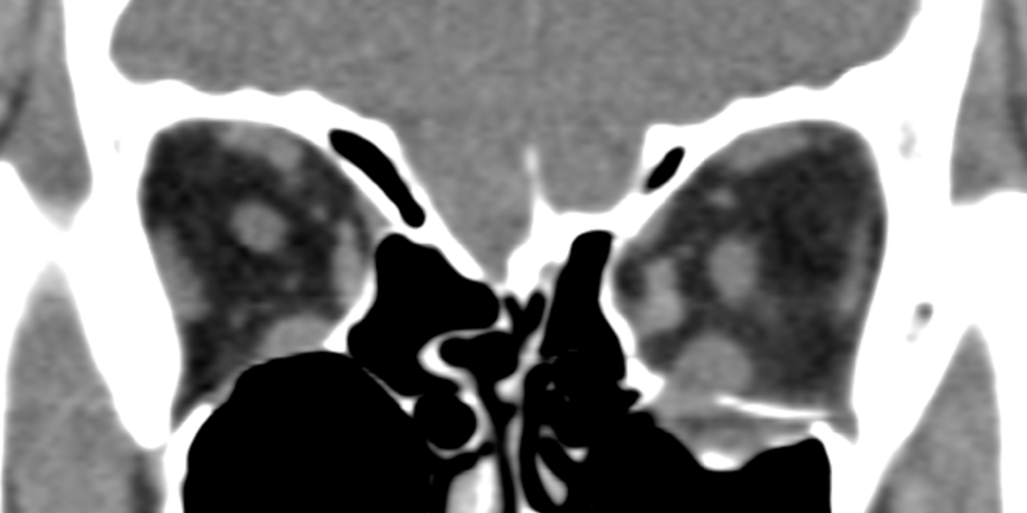
MRI shows a tumor larger than the eye in the posterior part of the eye; both T1 and T2 have similar signal intensity as the vitreous cavity. The border is clear. The diameter of the tumor is about 35 mm. How would you remove this tumor?
I chose to approach through a lateral canthotomy incision.
I started from lateral canthotomy. Cut into until periosteum, and then removed lateral wall of orbit.
The key of orbital tumor removal is how to use the malleable retractors.
Using 2 malleable retractors, separate the tumor from orbital tissue, and then, remove it.
3 month post-operation
The tumor was successfully removed and vision was restored.
Because of the very large tumor, the eye is rather concave after removal.
Comparison of before and after surgery.
The upper row is preoperative and the lower row is postoperative. You can see that the huge tumor was removed and no scar remains on the skin. Compared to before, the protrusion of the eyeball has improved and the vision, which was almost blind, has recovered to almost normal. Obviously, her quality of life improved due to aesthetic change.
Surgery video
Explanatory video of myocone intraorbital tumor removal Occulofacial Clinic Tokyo Dr. Tomoyuki Kashima
*This is an explanatory video of the actual surgery, so if you are not comfortable with surgical videos, please do not watch it.
Swinging eyelid approach
Next is the swinging eyelid approach. This is a technique in which an incision is made at the lateral canthus and the conjunctiva is directly incised to secure a large surgical field below the orbit.
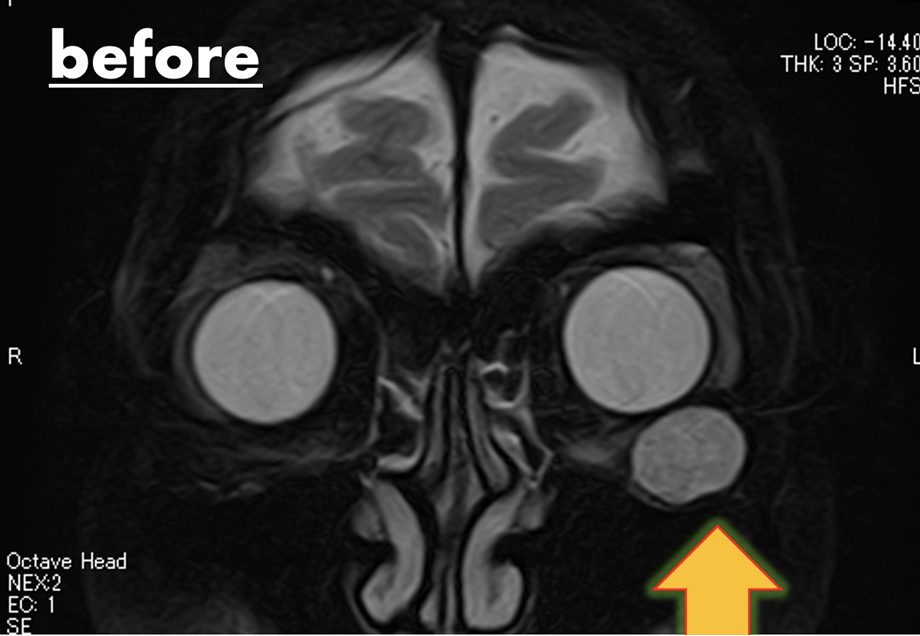
50 years old Female
Left extraconal orbital tumor
She is approximately 50 years old. A left orbital tumor is present below the eyeball. The increased size of the tumor has caused upward pressure on the eyeball, resulting in deviation.
This surgery was done with swinging eyelid approachIn Inferolateral quadrant, there is no important tissue, so I finished it in 18 mins. . I put this video on Youtube.
Postoperatively, differences in left and right eyelid shape and eye position have been resolved.
After surgery she regained symmetrical eyes aesthetically.
Upper eyelid crease
The next approach is upper eyelid crease incision.
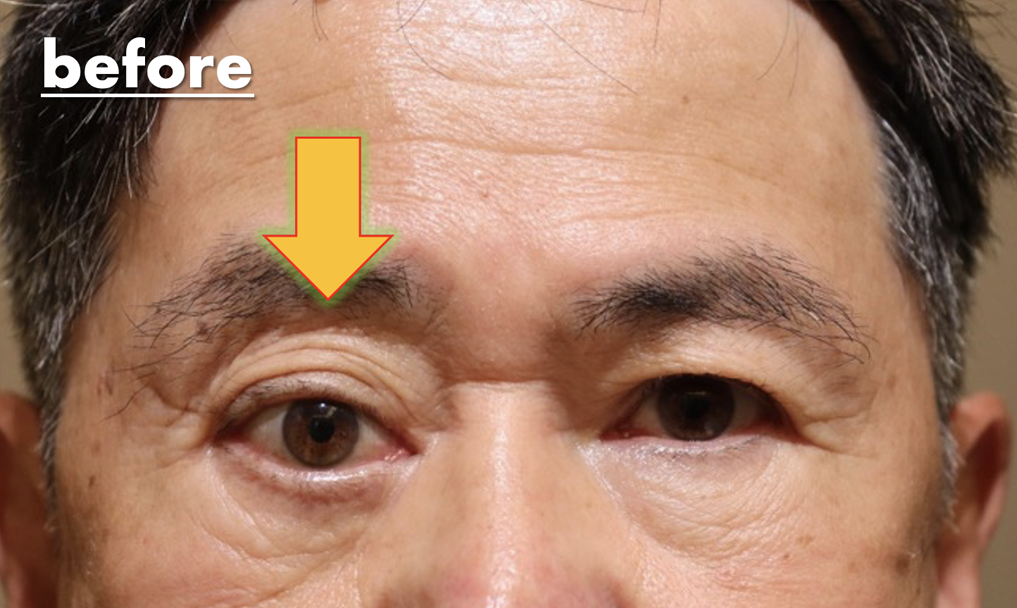
Approximately 70 years old Male
Right lacrimal grand tumor
The right eye is compressed by the tumor, causing not only ocular protrusion but also downward deviation of the eyeball.
Right Lacrimal gland tumor
MRI shows a tumor in the lacrimal gland area of the right orbit, compressing the eye.
I choose lid crease approach. Dissecting into the periosteum and expose bone.
And then, after bone removal, I removed lacrimal gland tumor.
Lacrimal gland tumor have loose adhesion laterally and superiorly, so you should start with that area.
It has tight adhesion inferiorly and medially, I recommend to loosen posterior side of lacrimal gland and dislocate it.
After tumor resection, ocular protrusion and downward deviation of the eyeball improved. But he developed and blepharoptosis.
Comparison of before and after surgery.
It can be seen that the preoperative protrusion of the eyeball has aesthetically improved.
The tumor has stretched the levator aponeurosis, resulting In a blepharoptosis.
This will be fixed by aponeurotic repair.
Please feel free to contact us first.
Our hospital strives to perform surgeries that minimize the burden on patients, such as post-operative pain and scars, more than any other medical institution in Japan. Please do not hesitate to contact us.
The cause of enophthalmos is Orbital Fracture, Enophthalmos after inadequate fracture repair and Congenital exophthalmos (by nature).
Orbital fracture
Enophthalmos with Orbital strut fracture
This patient have severe Enophthalmos with Orbital fracture
Enophthalmos with Orbital strut fracture
And this patient has enophthalmos with Orbital fracture too.
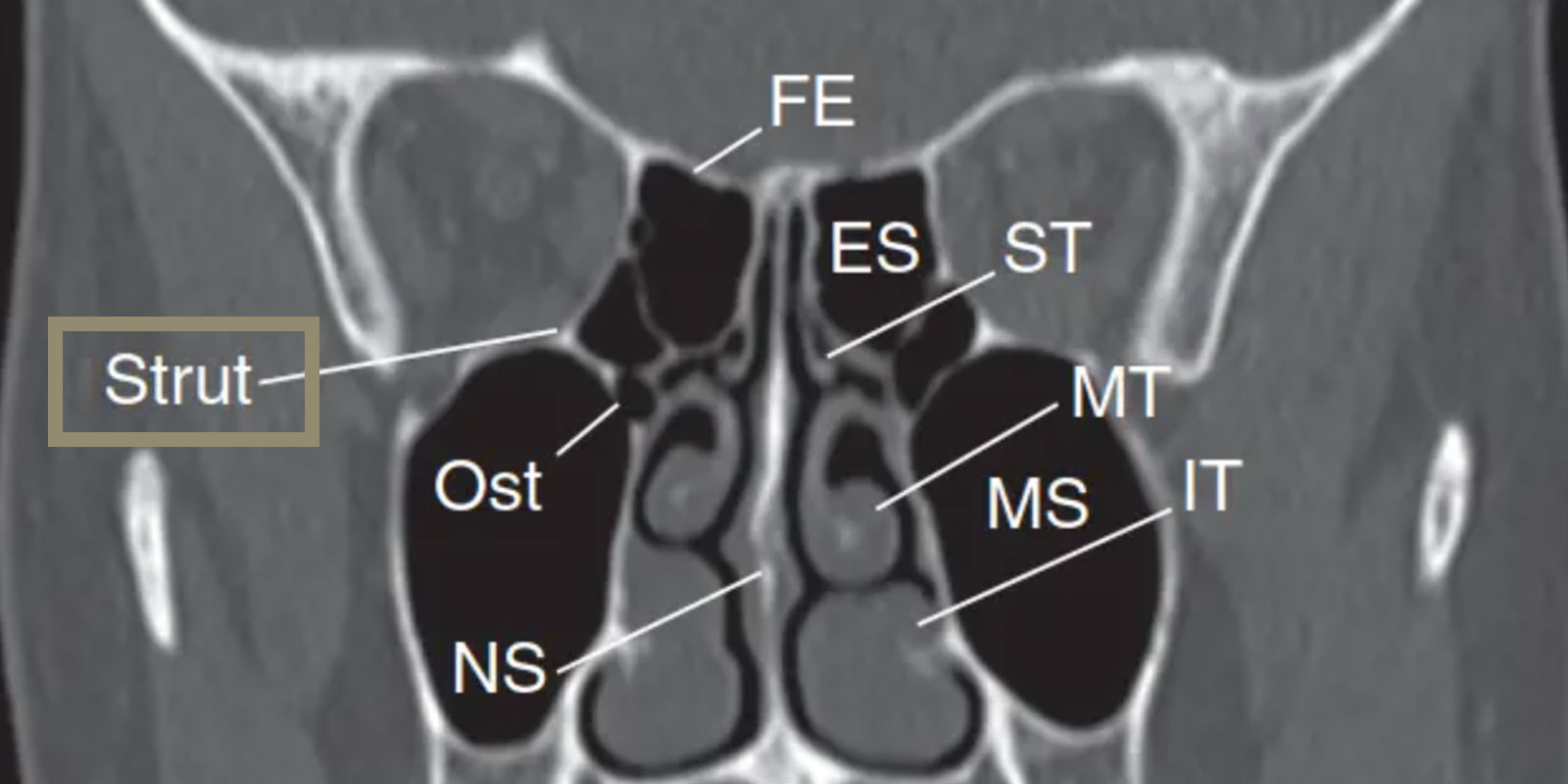
Surgeon must think about Orbital strut
Orbital strut is a supporting structure between medial wall and floor.
Break of orbital strut cause severe enophthalmos.
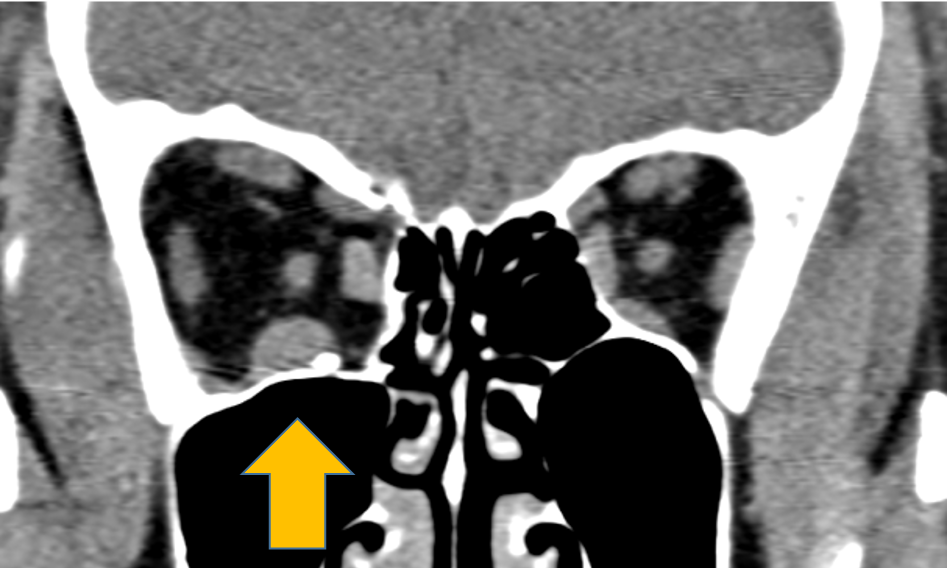
Must check the location of orbital strut before surgery.
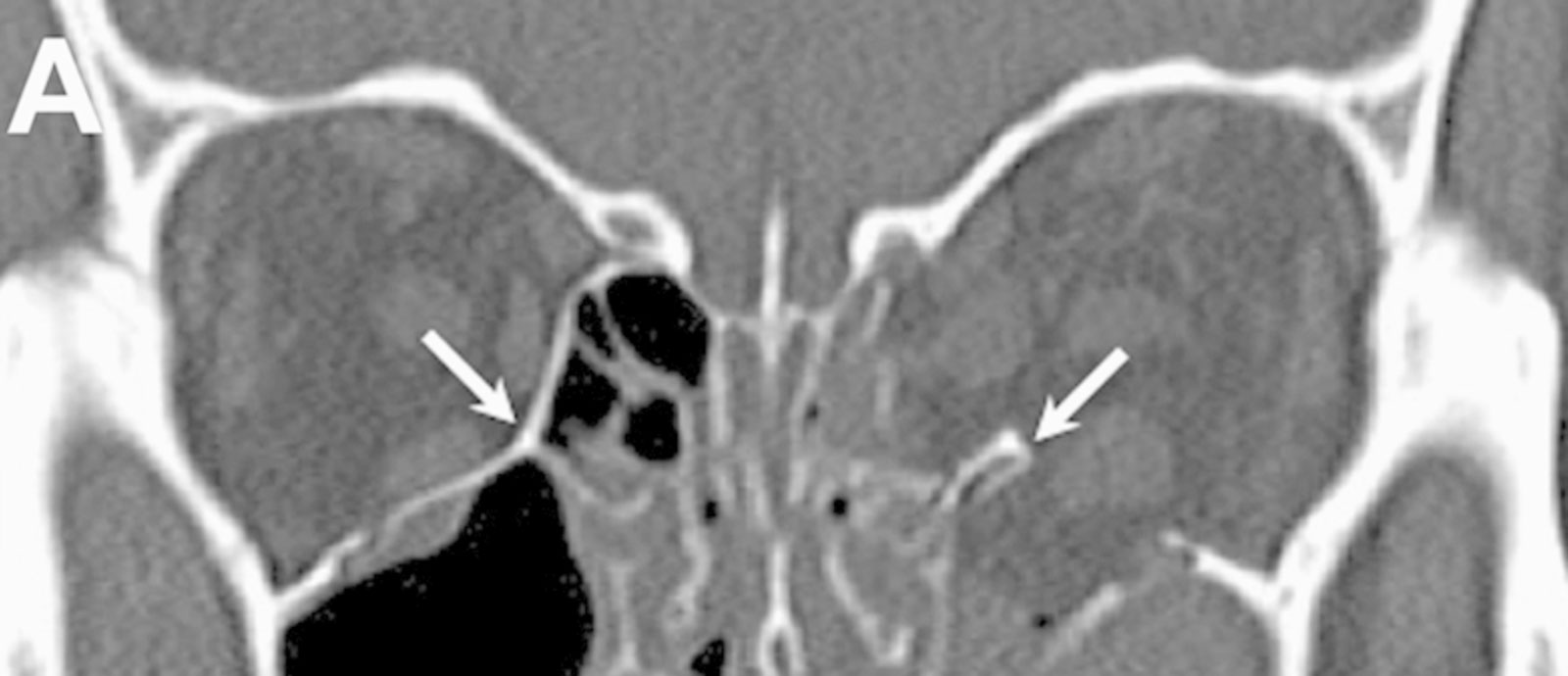
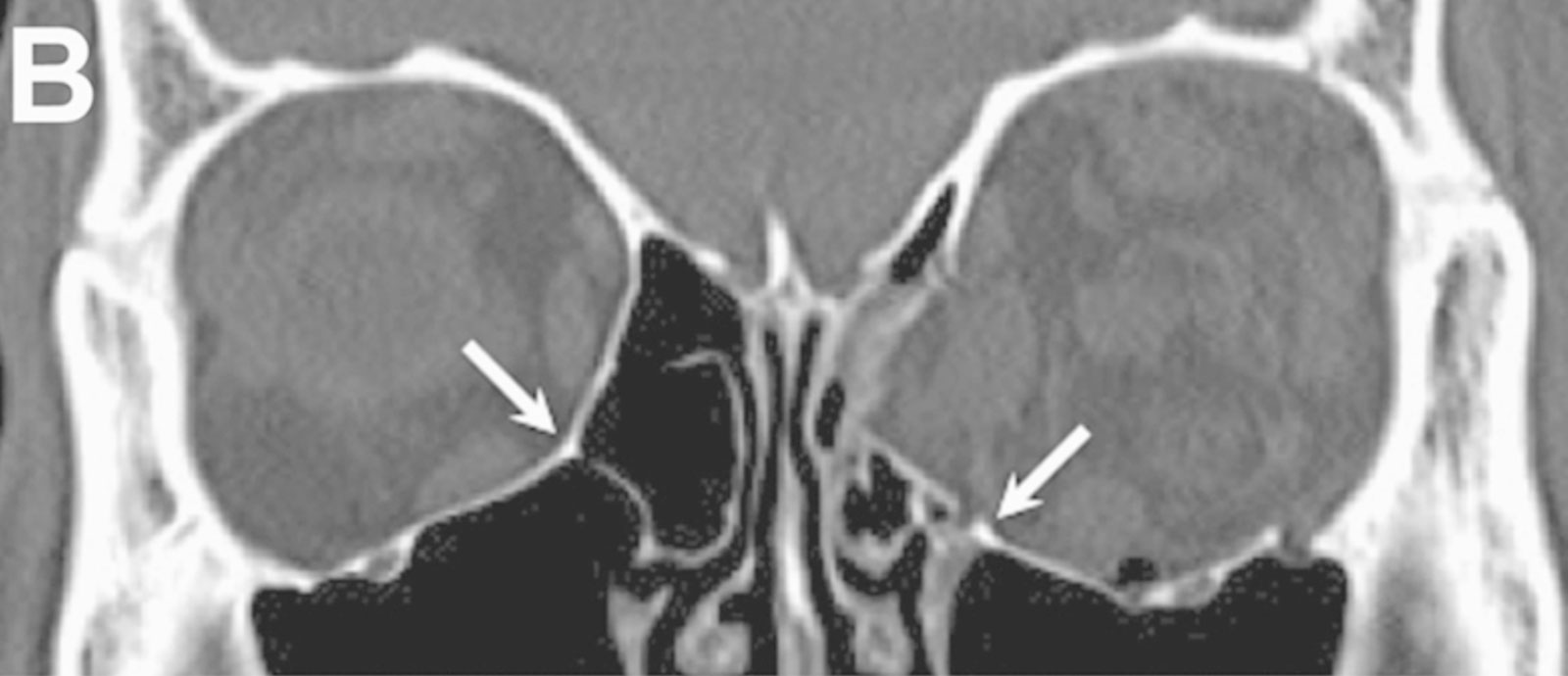
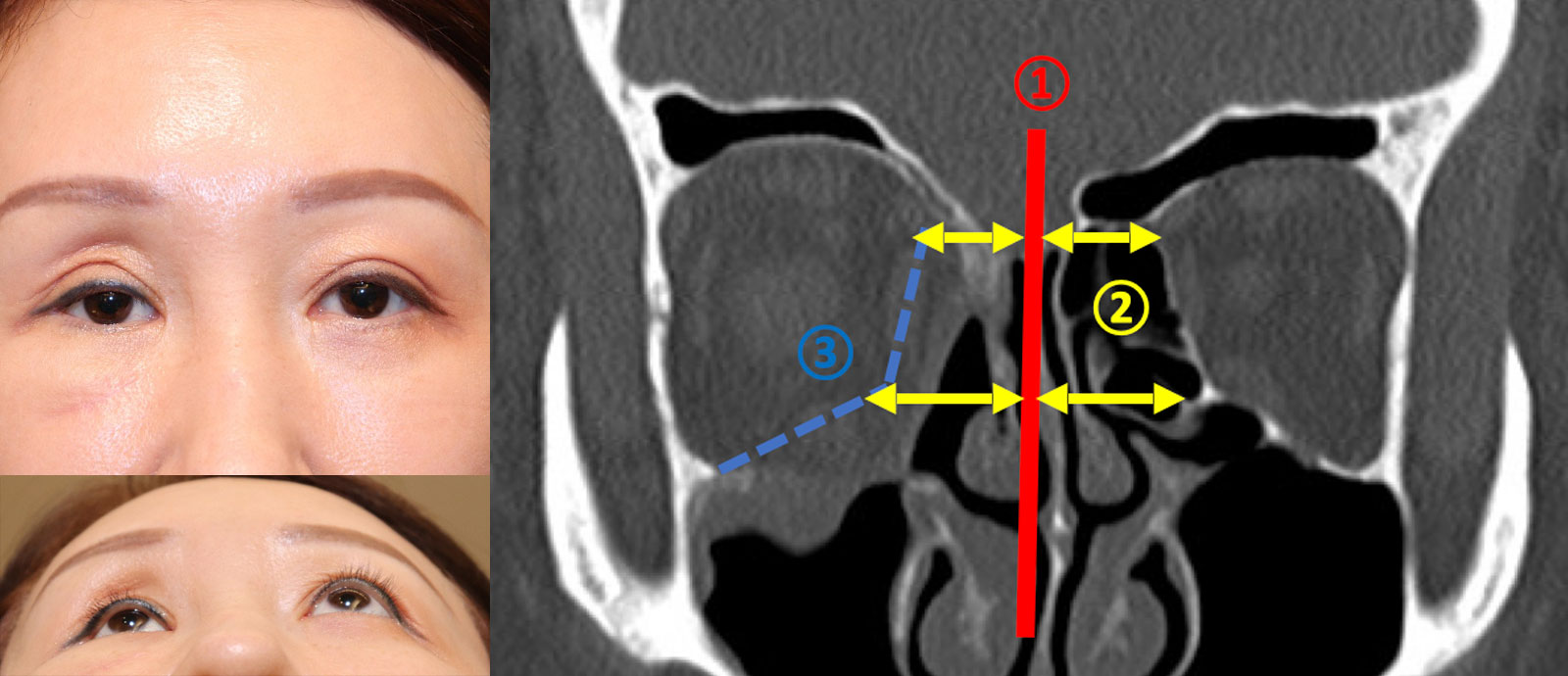
In the A, orbital strut remains although medial wall and floor is broken.
But in B, orbital strut, medial wall and floor, all structure is broken.
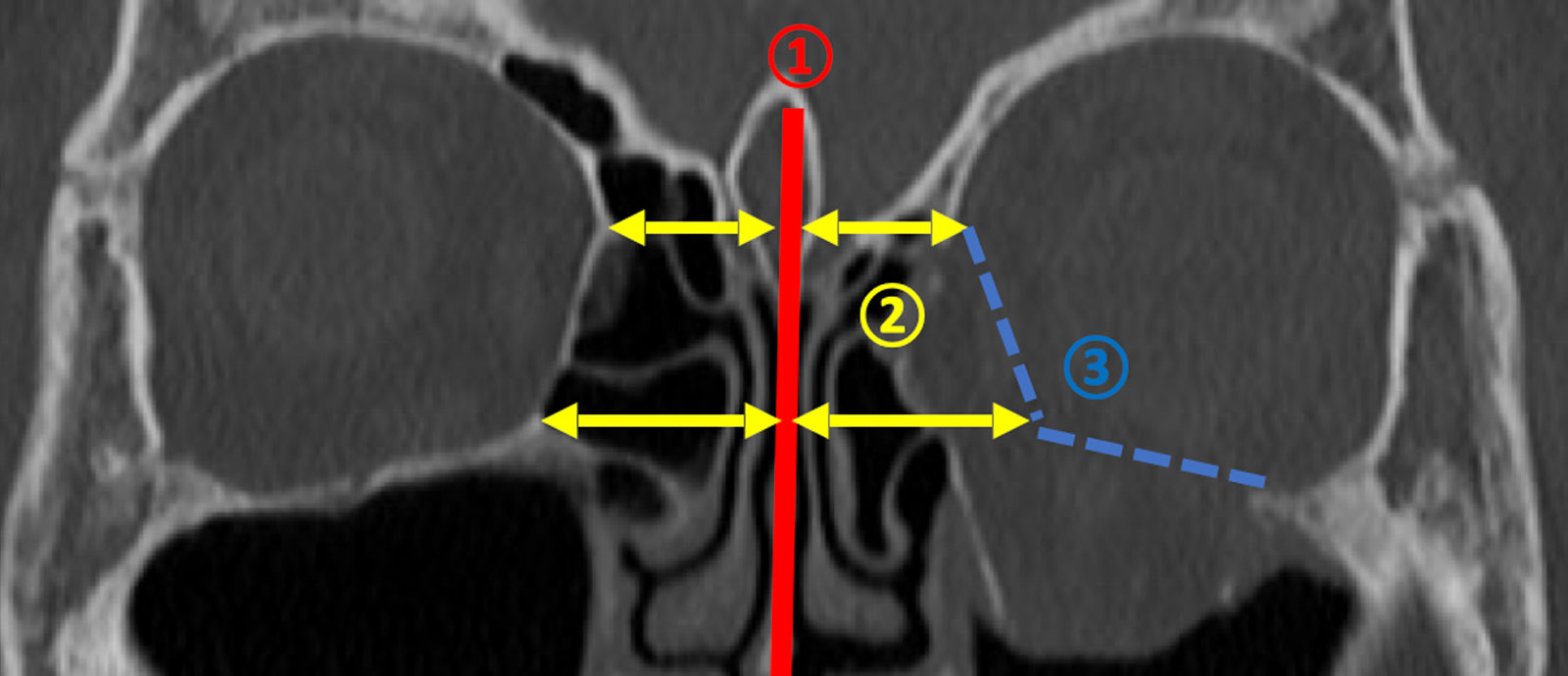
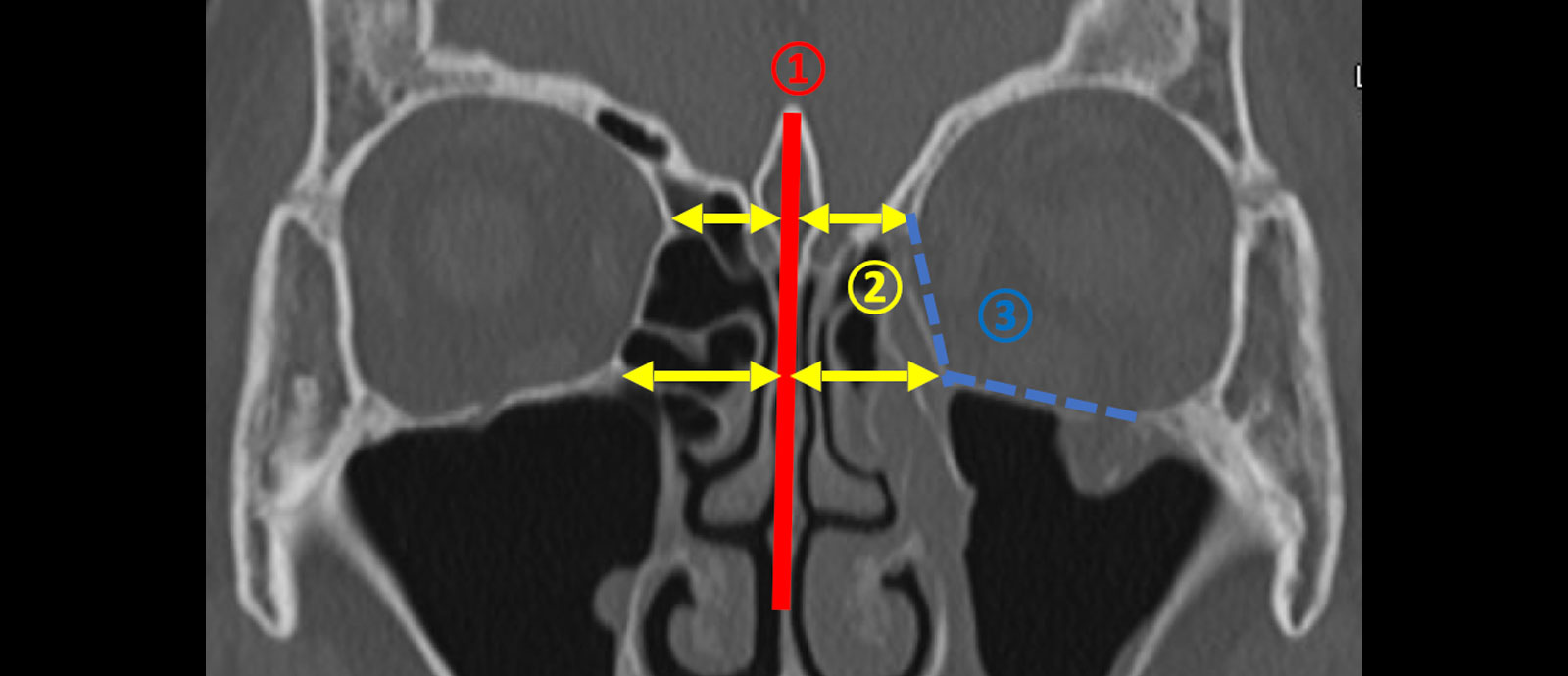
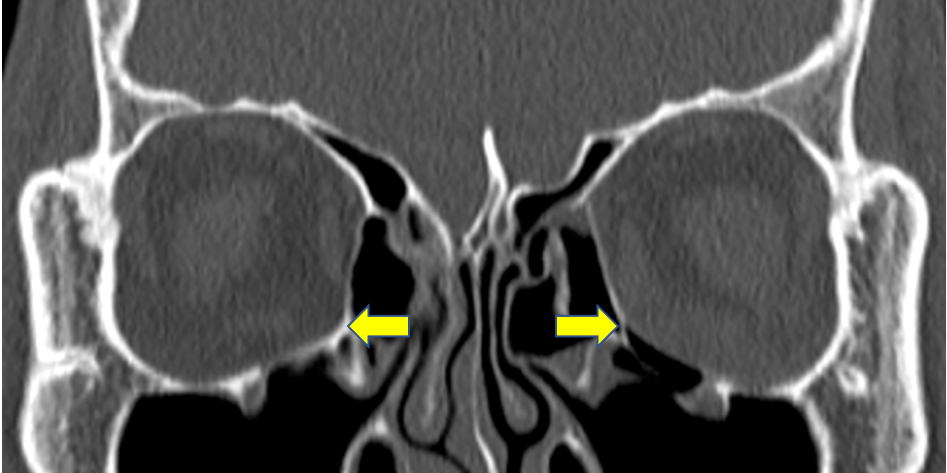
Key for preoperative assessment
Consider whether the shape of the right and left orbit is symmetrical with the nasal septum as the center.
Especially, you need to check the location of orbital strut.
Check the location of orbital strut, medial wall and orbital floor.
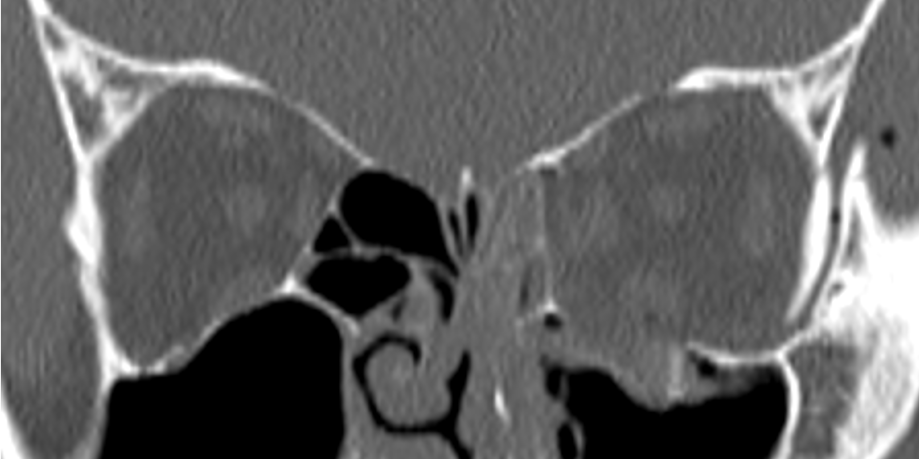
Assessment of orbital reconstruction by ENT surgeon.
This is another case after orbital reconstruction by ENT surgeon.
The surgeon removed orbital bone, so orbital strut disappeared.
We use transconjunctival approach for all cases.
No.1 No scarring on skin
No.2 Only 1-2 stiches for closure
No.3 Totally short operating time
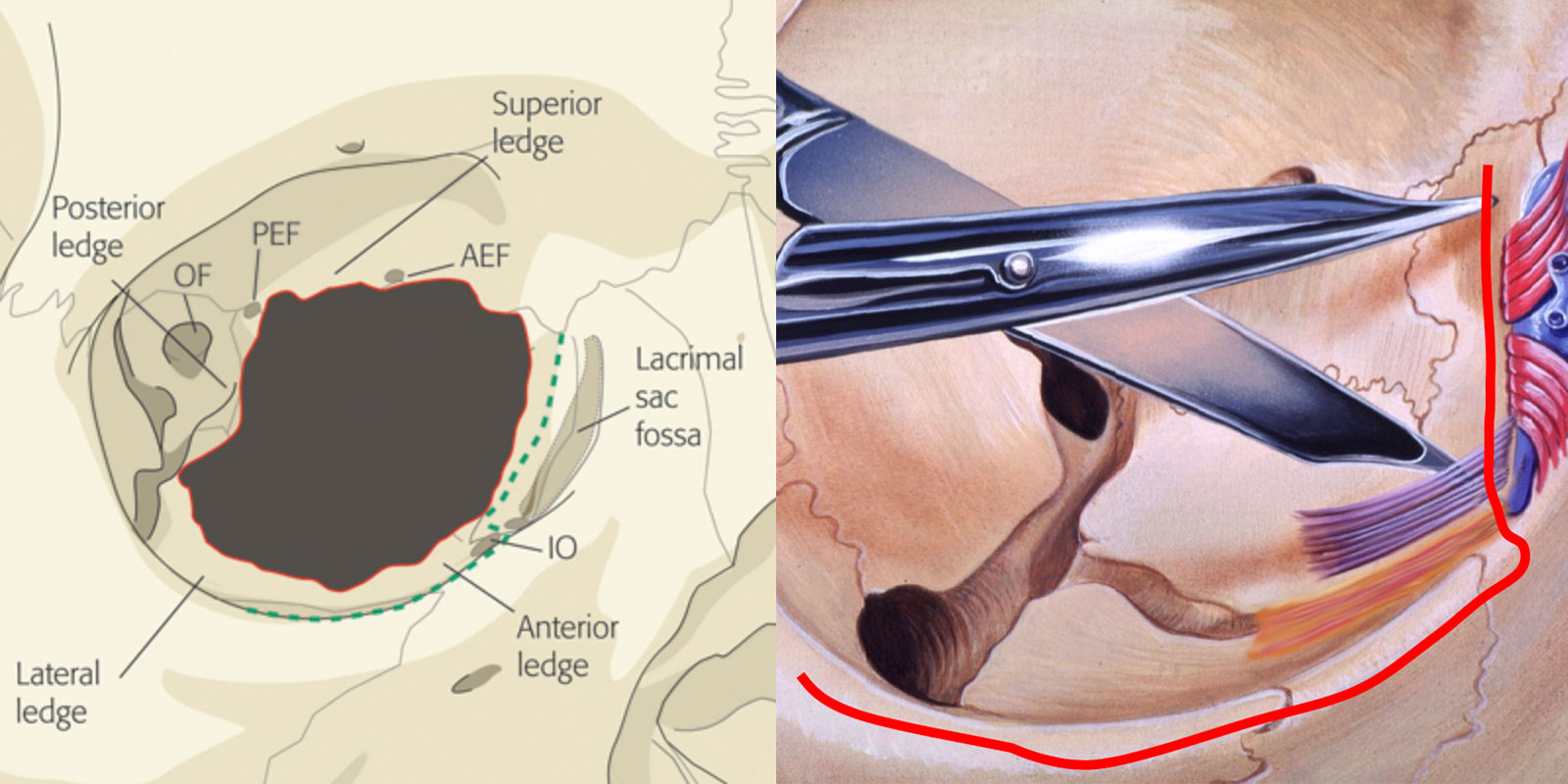
For reconstruction of orbital strut, we release muscle tendon of inferior oblique muscle.
For reconstruction of orbital strut, we always release muscle tendon of inferior oblique muscle.
After this, you can see medial wall and floor in the same view and insert big plates.
Conversely, without releasing inferior oblique, you cannot see both walls in the same view and cannot insert big plate.
Paper model of reconstructing medial wall and floor
This is paper model of reconstructing medial wall and floor by one plate.
We also use the other supporting plates if needs.
Orbital fracture CASES
CASE.1
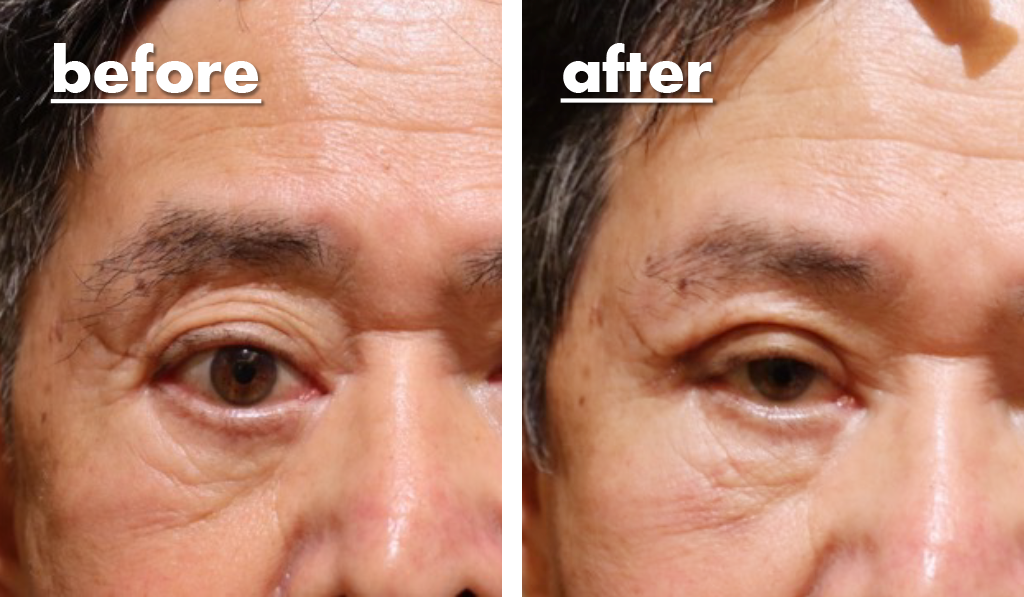
Severe enophthalmos on the left
This patient has severe enophthalmos on the left. He was just observed until being this condition.
Orbital strut fracture
He had orbital fracture including orbital strut and medial wall and floor. Postoperatively, the position of orbital strut become symmetrical also medial wall and floor too.
The left enophthalmos was recovered to the normal after surgery.
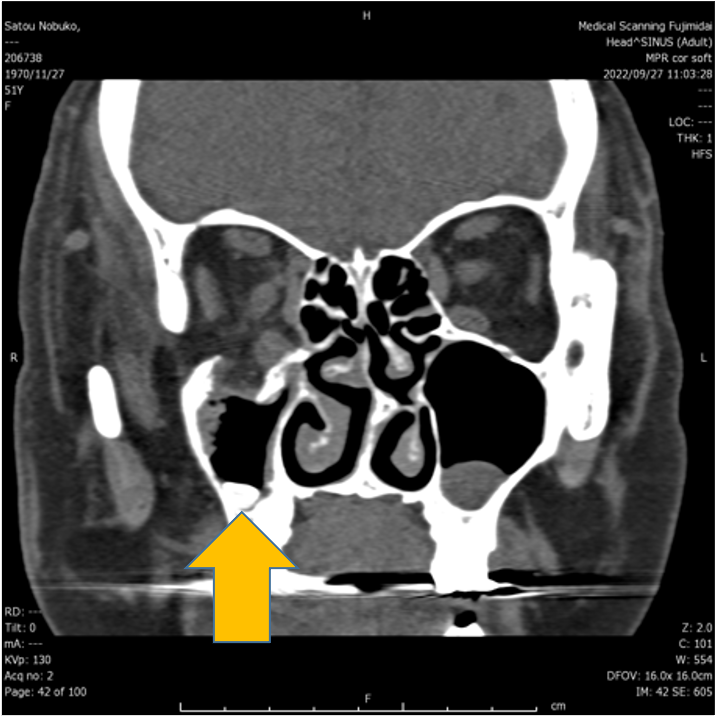
CASE.2
Left enophthalmos on left
This patient has left enophthalmos on the left
Orbital strut fracture
On CT scan, orbital strut including medial wall and floor was broken. So we performed repairing surgery. Postoperatively, the position of orbital strut become symmetrical.
Before surgery, enophthalmos and superior sulcus exists on the left, but it disappeared after surgery.
30 years old female
Revision after ENT surgeon’s repair
This case had severe enophthalmos because ENT surgeon removed all orbital bones before using balloons.
Her right orbit has enlarged due to lack of supporting tissue. So I dissect between orbital tissue and nasal mucosa and inserted the plates. After surgery, the position of orbital strut become symmetrical.
When you look at her right eye, it is very symmetrical after surgery although it was asymmetrical before surgery.
Also She can put make up after surgery, he cannot do it before surgery.
For congenital enophthalmos
Filler injection into DEEP orbit
Aesthetic hyaluronic acid is a drug injected primarily into the face.
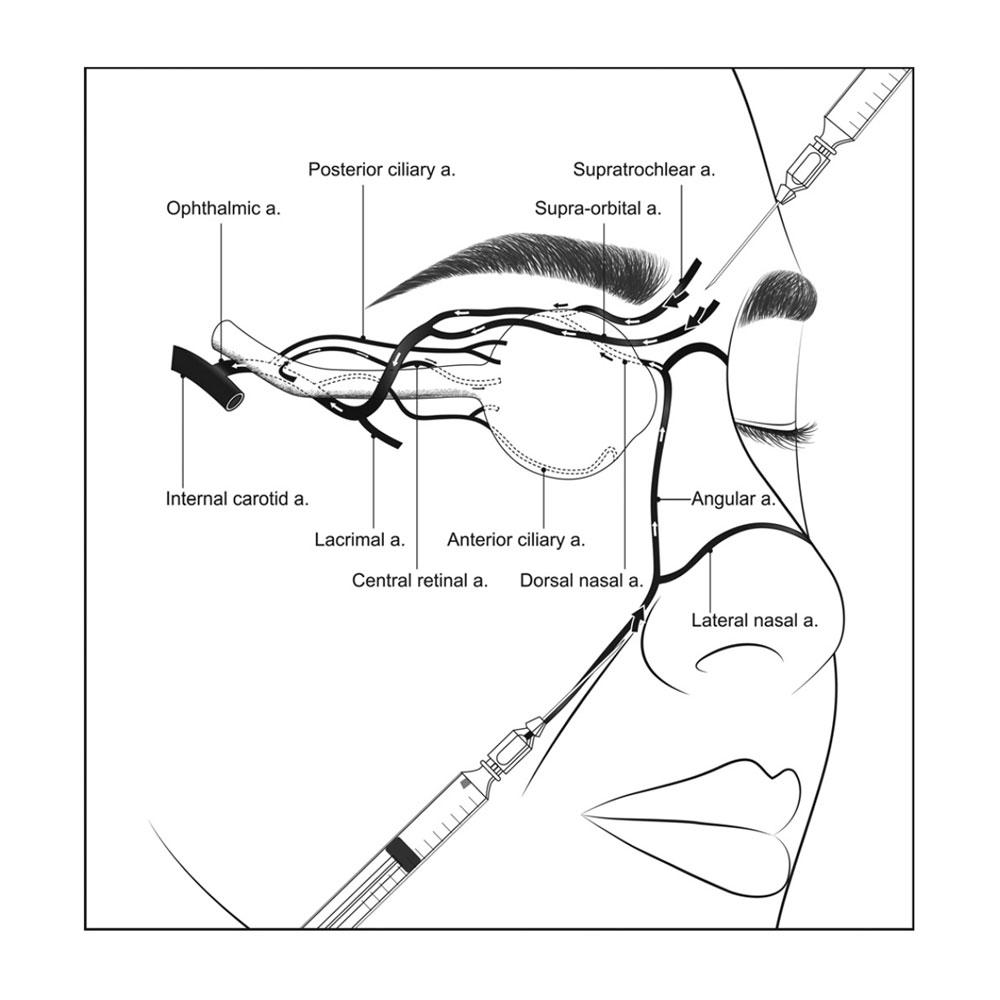
Complications include arterial occlusion, which can cause skin atrophy and necrosis. Rarely, it flows back into the ophthalmic artery, causing central retinal artery occlusion, or into the internal carotid artery, causing cerebral infarction.
Although such complications discourage the use of hyaluronic acid injections into the orbit, our clinic specializes in orbital surgery, and based on our knowledge, we have been injecting hyaluronic acid deep into the orbit for patients who wish to have it done.
Ophthalmic artery occlusion(OAO)
Iatrogenic retinal artery occlusion caused by aesthetic facial filler injections. Am J Ophthalmol. 2012
Iatrogenic occlusion of the ophthalmic artery after aesthetic facial filler injections: a national survey by the Korean Retina Society. JAMA Ophthalmol. 2014
Cerebral Angiographic Findings of Aesthetic Facial Filler-related Ophthalmic and Retinal Artery Occlusion. J Korean Med Sci. 2015
Fundus artery occlusion caused by aesthetic facial injections. Chin Med J (Engl). 2014
A Novel Hypothesis of Visual Loss Secondary to Aesthetic Facial Filler Injection. Ann Plast Surg. 2015
The mechanism of OAO after filler injection is…
It is caused by filler mistakenly injected into the angular ophthalmic artery or other arteries that goes against the flow of the artery and reaches the deepest part of the orbit, entering the ophthalmic artery.
So, the filler was injected into some artery mistakenly, and then, filler go deep inside the artery retrogressively, and at the junction of ophthalmic artery, the filler turned toward eyeball progressively in ophthalmic artery.
However, this is not a problem of ORBIT
So I think, To treat congenital enophthalmos, Is there any technique safely inject filler into deep orbit.
What we should consider is Anatomy and technique.
Anatomy
Technique
About anatomy
About anatomy, I had 2 questions.
Where is the location of ophthalmic artery?
How far is the orbital apex?
How far is it?
The depth of orbital apex is reported to be 42 mm. It is so far.
Actually, you do not have a sharp needle which can deliver the filler into the apex even it is very big needle.
If it can reach…
If it can reach, it can make damage to ophthalmic artery, central retinal artery and optic nerve.
Technique
How difficult it is to get into the retrobulbar space.
If the eyeball is perforated, there is a great possibility of blindness.
There are techniques that can anesthetize the eyeball with a blunt needle
Recently, ophthalmologists avoid retrobulbar injection with a sharp needle.
My method
To deliver hyalonic acid gel into deep orbit safely.
Use a 24-gauge cannula needle. Remove the outer casing and cut away the plastic part at the base of the needle.
Return the needle and insert the cannula needle into the skin. Stop at a point shallow enough not to pierce the eyeball, and remove the injection needle, leaving the outer casing in place.
An aesthetic-treatment 40 mm blunt needle is then placed inside to penetrate deeper, safely reaching a depth of approximately 40 mm.
Congenital enophthalmos cases
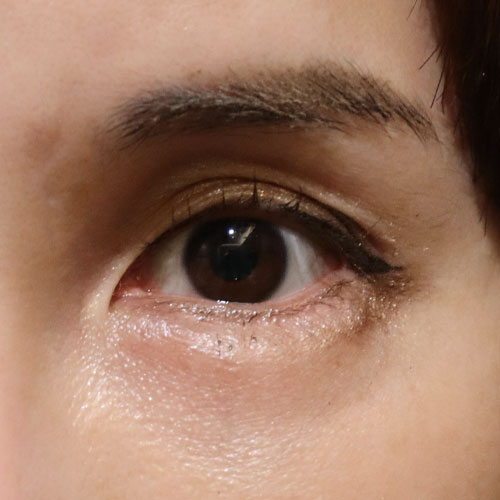
You can see the change of two eyes. The eye looks more natural and severe enophthalmos reduced.
The patient was pleased very much because our clinic is the only one which aesthetically treat congenital enophthalmos.
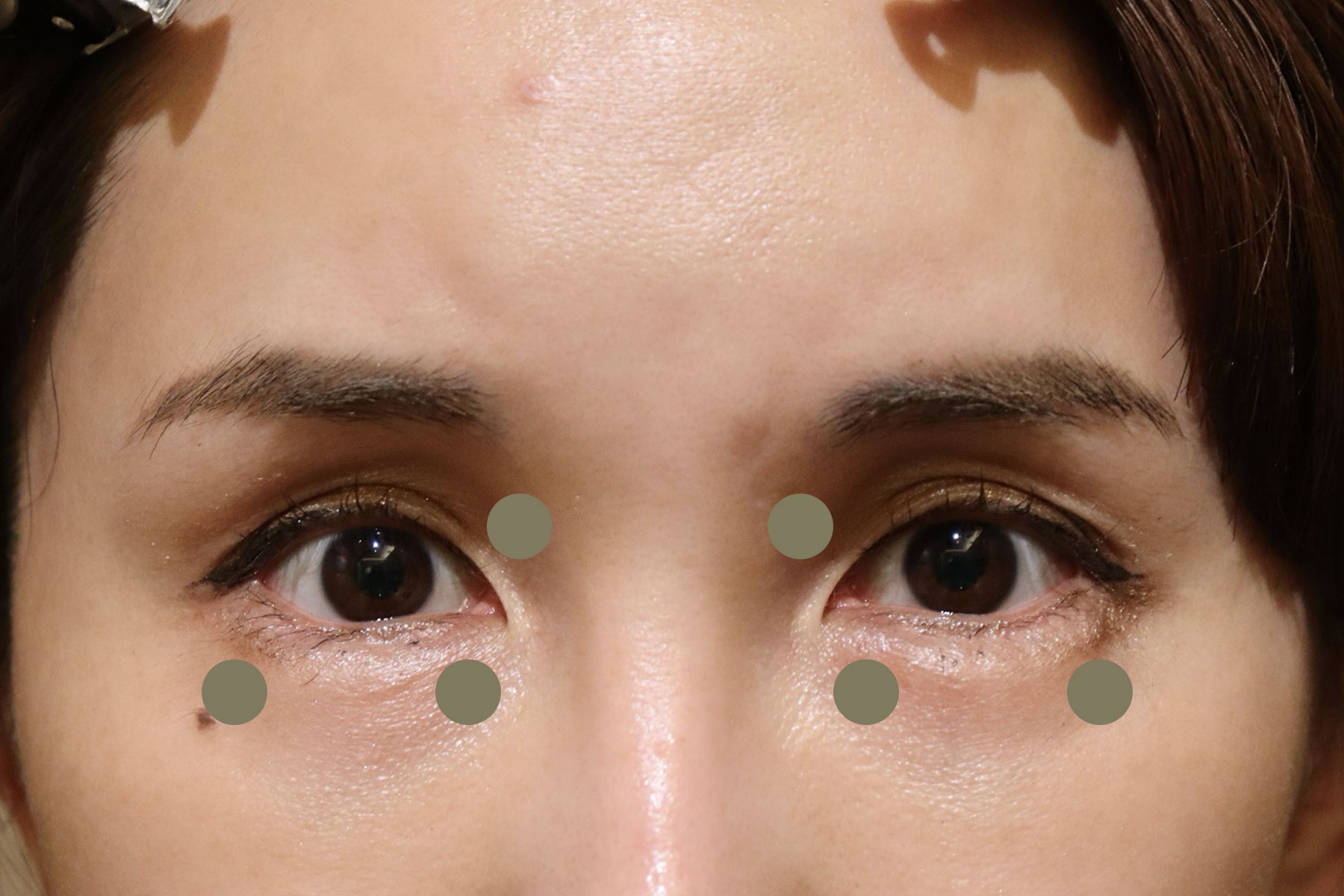
Case1: 42y.o. female 1.5cc for each orbit
The first case is 42 y.o. female.
I injected 1.5cc hyalonic acid gel into the deep orbit from 3 locations.
Obviously, shadow in upper eyelid decreased after the injection.
You can see the change of two eyes. The eye looks more natural and severe enophthalmos reduced.
You can see the change of two eyes. The eye looks more natural and severe enophthalmos reduced.
The patient was pleased very much because our clinic is the only one which aesthetically treat congenital enophthalmos.
Case2: 34y.o. female. 1.1cc for both orbit
The second case visit us also complaining about congenital enophthalmos.
Actually, I do not think she have enophthalmos, but she eager to do filler injection.
After the injection of 1.1cc hyalonic acid gel into the orbit, the eyes become bigger, and the sulcus of both eyes disappeared.
Comparing case 1, the amount of filler is less, so the change is less too.
The eyes become bigger, and the sulcus of both eyes disappeared.
The eyes become bigger and the sulcus of both eyes disappeared.